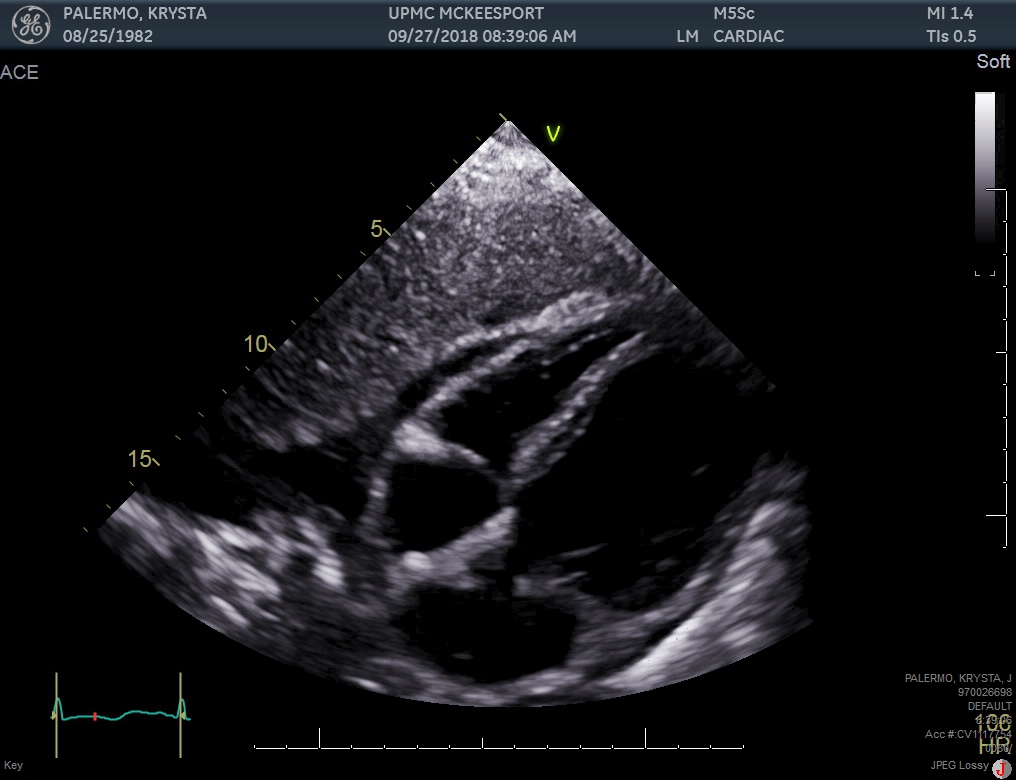
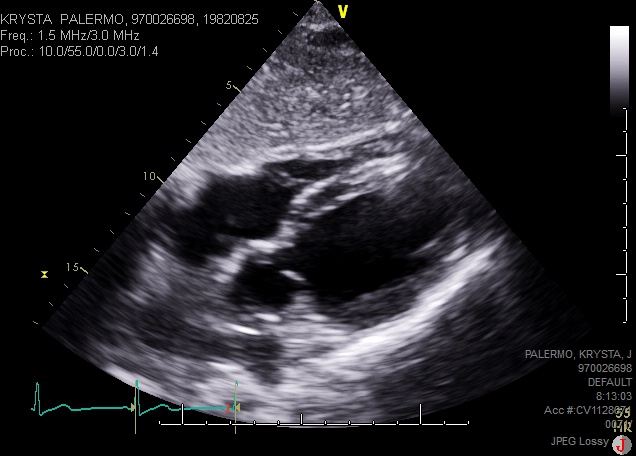
Case Presentation: A 36 years old female with past medical history of IV drug abuse, presented with dyspnea, nasal congestion, tactile disturbances, diarrhea, body aches and generalized weakness for 1 day. She was recently treated for tricuspid valve endocarditis. A Transthoracic Echocardiogram (TTE) obtained at that time showed ejection fraction (EF) of 55-60%. On presentation, vital signs were remarkable for tachycardia and tachypnea. Physical examination demonstrated bibasilar crackles and peripheral edema. ECG showed sinus tachycardia. Chest X-ray revealed pulmonary edema. CT angiogram did not show any pulmonary embolism or septic emboli. Her laboratory findings included BNP of 1070 pg/ml and troponin elevation of 2.030 ng/ml. Urine drug screen was positive for opiates and benzodiazepines. Infectious disease workup was negative. TTE revealed reduced EF of 10-15% and wall motion abnormalities consistent with apical ballooning and hypokinesis of basal segments of left ventricle. InterTAK diagnostic score was 85, showing 99% probability of takotsubo cardiomyopathy. Cardiac catheterization was done that did not show critical coronary artery obstruction. Left ventriculogram revealed apical ballooning with preserved contraction of the base of the ventricle. The patient was diagnosed and treated for heart failure due to takotsubo cardiomyopathy caused by opiate withdrawal. Repeat TTE after 3 weeks showed EF of 55-60% and complete resolution of wall motion abnormalities.
Discussion: Takotsubo cardiomyopathy is a stress-related transient left ventricular dysfunction, typically featuring apical ballooning, in the absence of angiographic evidence of coronary artery disease or acute plaque rupture. Opioid withdrawal is a hyperadrenergic state that can manifest as physical and emotional stress. This high adrenergic state can lead to diffuse catecholamine-induced coronary spasm or microvascular dysfunction, resulting in myocardial stunning, leading to takotsubo cardiomyopathy, as in our case.
Conclusions: In a patient with history of opioid use, presenting with withdrawal symptoms, new-onset systolic dysfunction and apical ballooning with basal hypokinesia on TTE, takotsubo cardiomyopathy should be in the differential.