Background: Multi-visit patients (MVP) tend to represent a small portion (< 5%) of all admitted patients, yet account for more than 40% of 30-day readmissions based on prior literature (1-2). Among our institution’s MVPs, Heart failure (HF) exacerbations are one of the top disease presentations accounting for 40% of 30-day readmissions in 2022. These patients are very complex with medical, behavioral, and social needs that have been under-addressed within the current system. Current post-discharge follow-up processes have been inconsistent in meeting the patient’s unique driver of utilization (DOU) of the healthcare system and have failed to address individual needs to reduce readmissions (3). As such, our study focused on MVPs with HF with the goal of reducing readmission rates by using a team-based approach to deliver patient-centered interventions based on their DOU using the “MVP method” as framework (4).
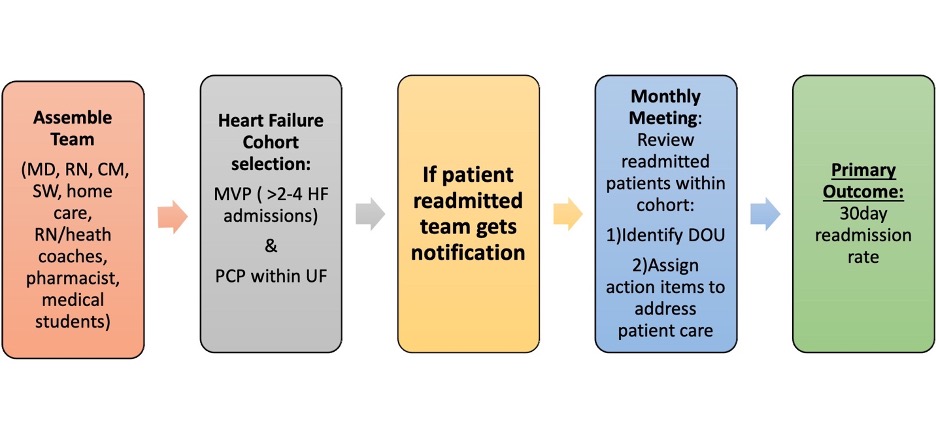
Methods: MVPs were selected if they had 2 or more admissions for HF within a 1-year period and had a primary care provider within our health system. The number of admissions was lowered from the traditional MVP definition of 4 admissions/year to identify patients earlier in the disease process. After the cohort was selected, the multidisciplinary team (medical students, physicians, nurses, case managers, discharge planners, home health care liaisons, pharmacists, RN-health coaches, and social workers) met monthly to monitor readmissions and review MVPs that were readmitted. During these meetings the DOUs were identified, and actionable tasks were assigned to address MVPs’ post-discharge needs. Examples of actionable tasks included pharmacy medication review, RN-Health Coach contact, and transitional care program setup. The goal was to deliver real-time interventions after the patient was discharged to prevent readmissions. Patients that qualified also received a HF discharge kit to help monitor their condition at home. Post-discharge measures were also monitored to ensure appropriate discharge follow up which included RN-health coach contact within 2 days and discharge appointment scheduling.
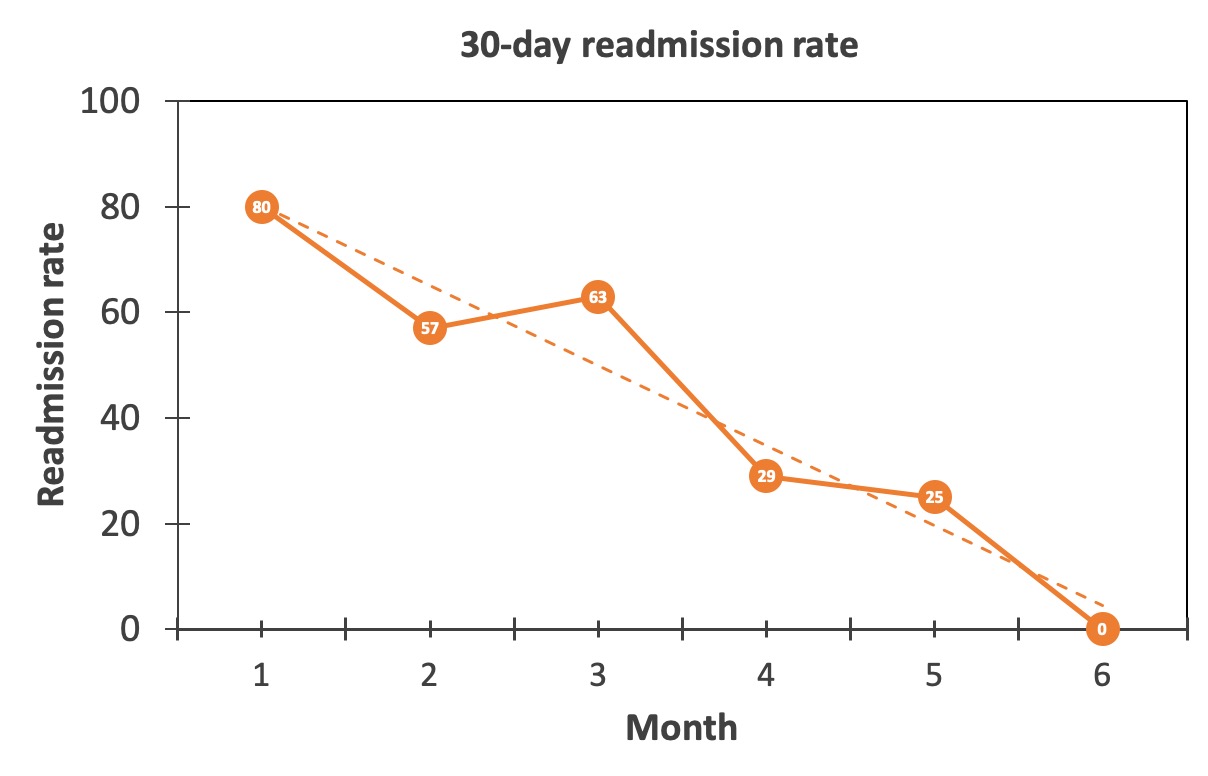
Results: The initial study was for a period of 6 months and included 21 patients. The top drivers of utilization identified were: chronic unstable baseline (56%), inadequate support and services (23%), and unaddressed goals of care/end of life (15%). The top actionable items identified were pharmacist medication review (n=16), RN Health Coach interventions (n=12), and Take Charge Transitions Program (n=8). Process measures showed RN-health coach contacting patient within 2 business days of discharge with an average 81%. Scheduling post-discharge follow up appointments within 7days averaged 69%. The 30-day readmission rate showed consistent decline with linear regression model RR2 adjusted 90.8% and p-value 0.002.
Conclusions: Using a team-based approach guided by DOU to deliver tailored interventions post-discharge shows promising results to help reduce readmission in MVPs with HF. Future directions include expansion of this approach with larger cohort which is now underway. Potential barriers include nursing turnover and sustainability. As such, we are exploring collaborations with our AI team to potentially streamline interventions such as AI-generated patient education tools. We are also working on expanding real-time intervention when patients are admitted instead of post-discharge, specifically the optimization of GDMT, as several studies have shown this is key in reducing readmission.