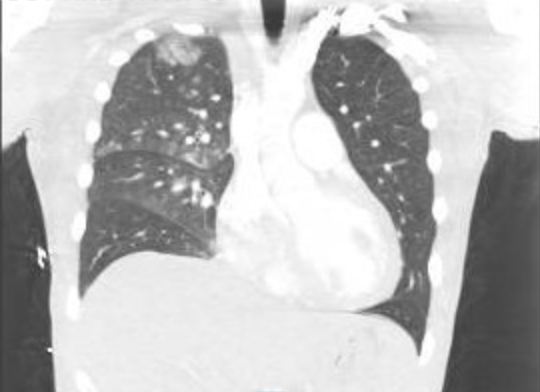
Case Presentation: A 31 year old male with no known medical history presented to the hospital with complaints of acute onset chest pain, shortness of breath and 30 lb weight gain. History was notable for a period of starvation with intake of exogenous testosterone, T3 and growth hormone prior to a bodybuilding competition followed by 3 days of binge eating and drinking before symptom onset. On presentation, he was febrile, tachypnic, tachycardic and hypoxic to 92% on 4L NC and uptitrated to 100% HFNC with O2 96%. Physical exam was positive for jugular venous distention, bibasilar crackles on lung exam, and generalized trace edema. EKG performed in the ED showed sinus tachycardia with HR 116 and no evidence of ST elevations or depressions and cardiac enzymes were notable for CK 3373 U/L, troponin T 3484.6 ng/L, and proBNP 1049 pg/mL. CTA showed ground glass opacities in the right lung with a small right pleural effusion but was negative for pulmonary embolism. TTE showed moderate global left ventricular systolic dysfunction with severe reversible diastolic dysfunction meeting criteria for stage III heart failure and EF 44%. Infectious workup otherwise was negative. Patient was initiated on furosemide, carvedilol and entresto. Patient showed improvement in oxygen status and was weaned off supplemental oxygen. The patient was found to have a pattern of central hormone deficiencies with high total testosterone, low FSH, low TSH, and low normal ACTH noted with an elevated prolactin. MRI of the pituitary was normal favoring a negative feedback system induced by hormone supplementation. This case highlights the adverse effects of exogenous steroid supplements and its potential to cause cardiac events.
Discussion: Cases of acute decompensated heart failure (ADHF) are seen routinely in internal medicine; most often with exacerbation due to noncompliance with salt restriction or development of arrhythmias and new onset commonly due to coronary artery disease or worsening hypertension. Our case is unique in that we saw new onset ADHF secondary to exogenous hormone supplementation. Hormones such as testosterone have been shown to cause inflammation and fibrosis in the setting of myocarditis. Hospitalists very commonly admit cases of ADHF as it contributes to 70% of cases of inpatient hospitalizations per year. This case demonstrated the importance of obtaining a thorough social history and reviewing all non-prescription supplements as a cause of a common medical presentation.
Conclusions: Here we present a common cause of hospitalization with ADHF with an atypical cause being steroid hormone supplementation for recreational activity. Our case demonstrates that obtaining a thorough social history can help with identification of uncommon etiologies to help tailor individual treatment and improve overall outcomes.