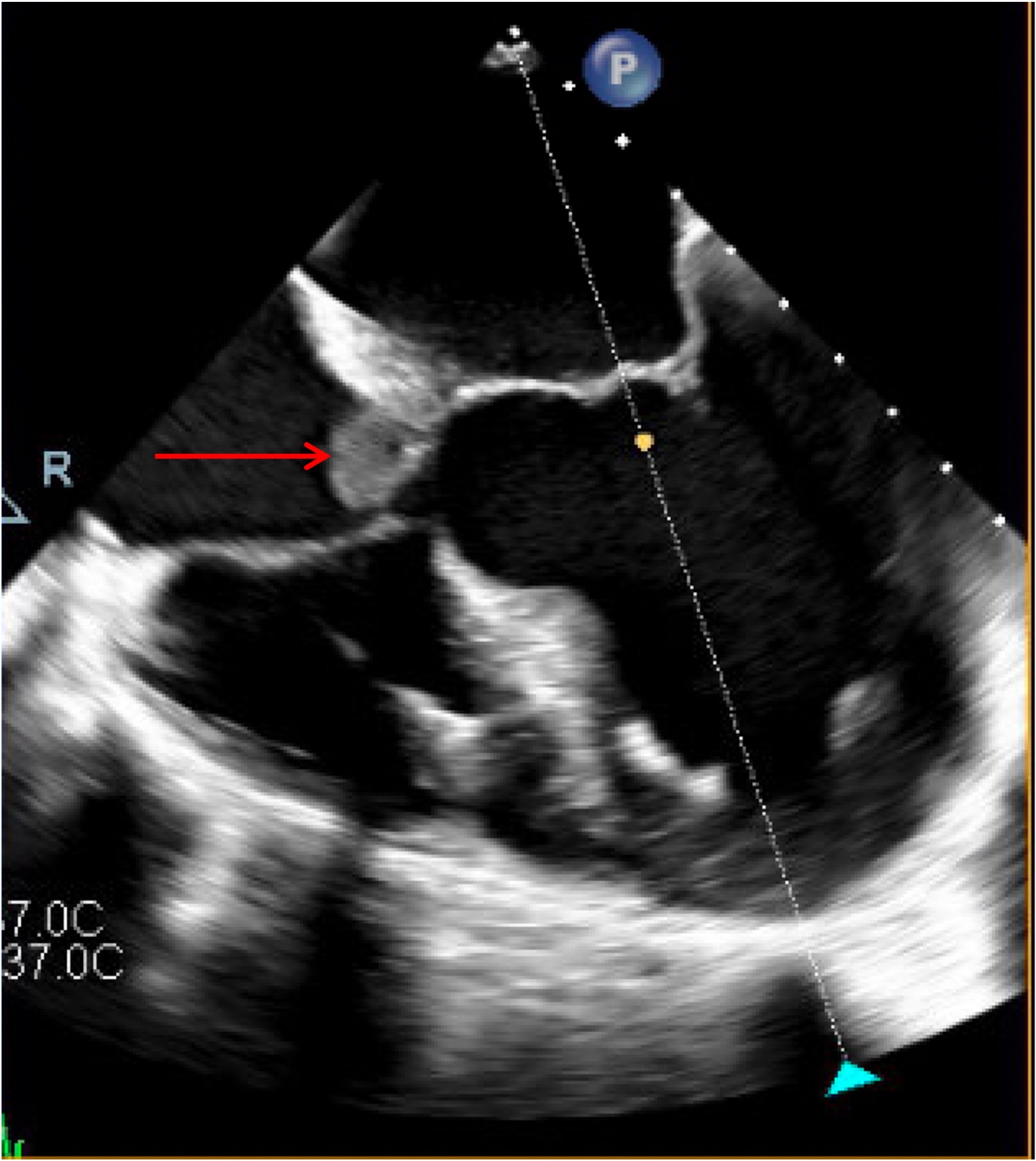
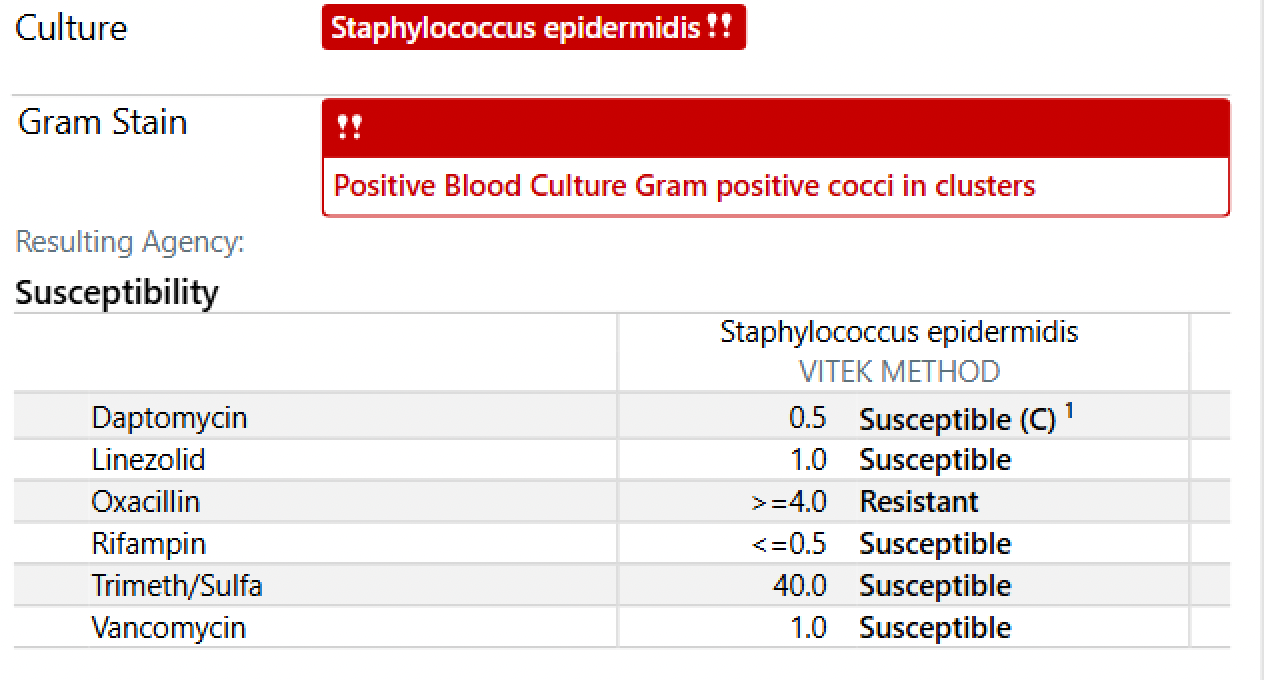
Case Presentation: A 76-year-old woman with prior bioprosthetic aortic valve replacement, coronary artery disease, chronic kidney disease on hemodialysis, and multiple comorbidities presented with acute left upper-extremity ischemia requiring thrombectomy. A single blood culture grew S. epidermidis and was considered a contaminant after rapid clearance on repeat testing. Ten days later, recurrent methicillin-resistant S. epidermidis (MRSE) bacteremia developed, and TEE demonstrated large vegetations on the prosthetic aortic valve with an extensive peri-aortic root abscess extending into the interatrial septum and right atrium, associated with partial valve dehiscence. Multidisciplinary evaluation deemed the patient at prohibitive surgical risk; she was managed palliatively with intravenous vancomycin. Despite therapy, bacteremia persisted, and she succumbed to progressive infection complicated by abscess fistulization into the right atrium.
Discussion: This case highlights the diagnostic challenges of coagulase-negative staphylococcal (CoNS) bacteremia in patients with prosthetic valves. S. epidermidis, traditionally regarded as a low-virulence contaminant, is now recognized as a leading cause of prosthetic valve endocarditis, driven by its biofilm-forming capacity and methicillin resistance. Even transient or single-bottle bacteremia may represent true infection in high-risk hosts, and misclassification can delay recognition of destructive disease. In this patient, initial dismissal of the positive culture preceded the development of a rapidly progressive peri-aortic abscess with intracardiac fistulization—complications well-documented in the CoNS endocarditis literature. Although homograft or allograft aortic-root replacement offers the best chance of cure, comorbidities often preclude surgery, and medical therapy alone rarely eradicates biofilm-mediated infection.
Conclusions: Staphylococcus epidermidis bacteremia should not be automatically labeled as contamination in patients with prosthetic valves or intravascular devices. Early repeat cultures, timely multimodal imaging, and multidisciplinary evaluation are essential. Definitive cure of MRSE PVE requires surgical source control; when surgery is not feasible, outcomes remain poor. This case underscores the need for heightened vigilance and early intervention to prevent catastrophic complications of CoNS prosthetic valve endocarditis.