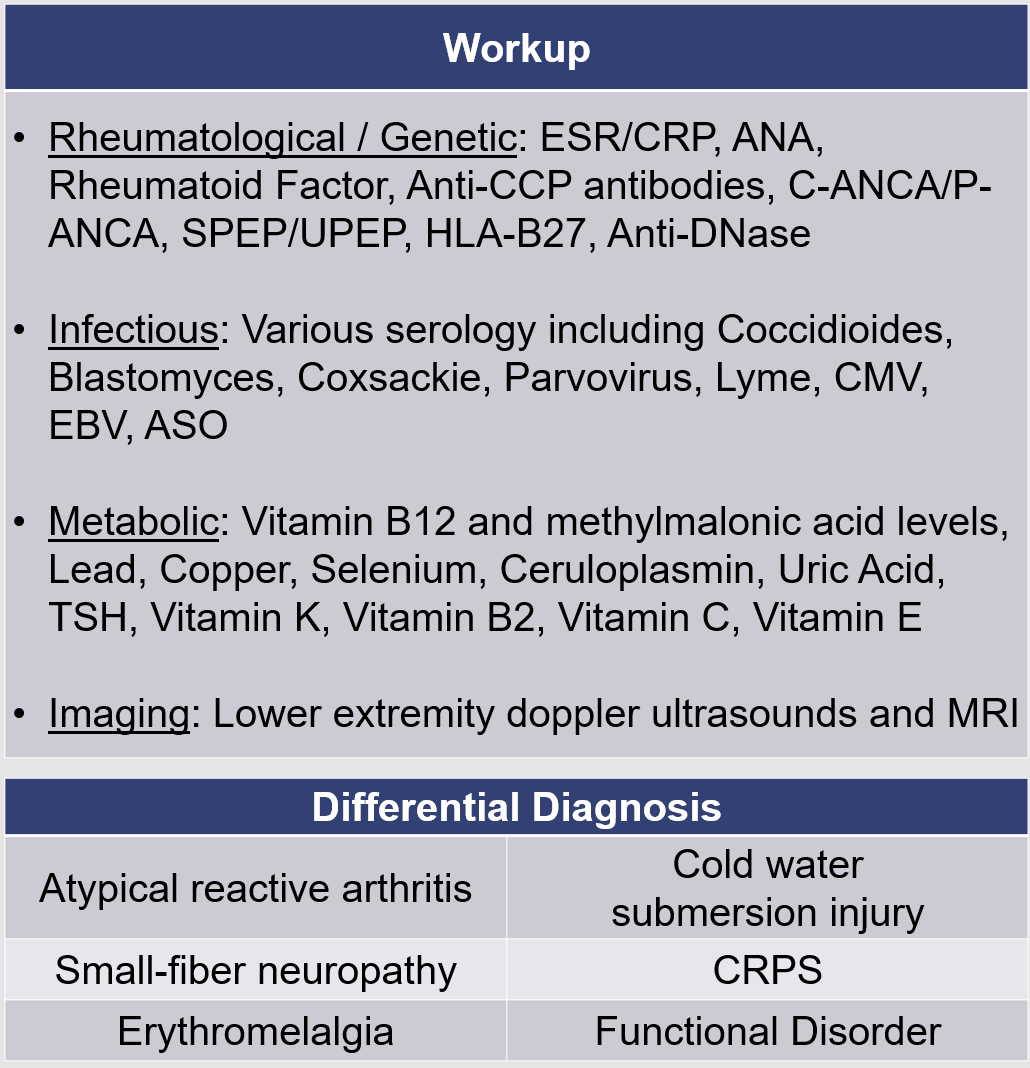
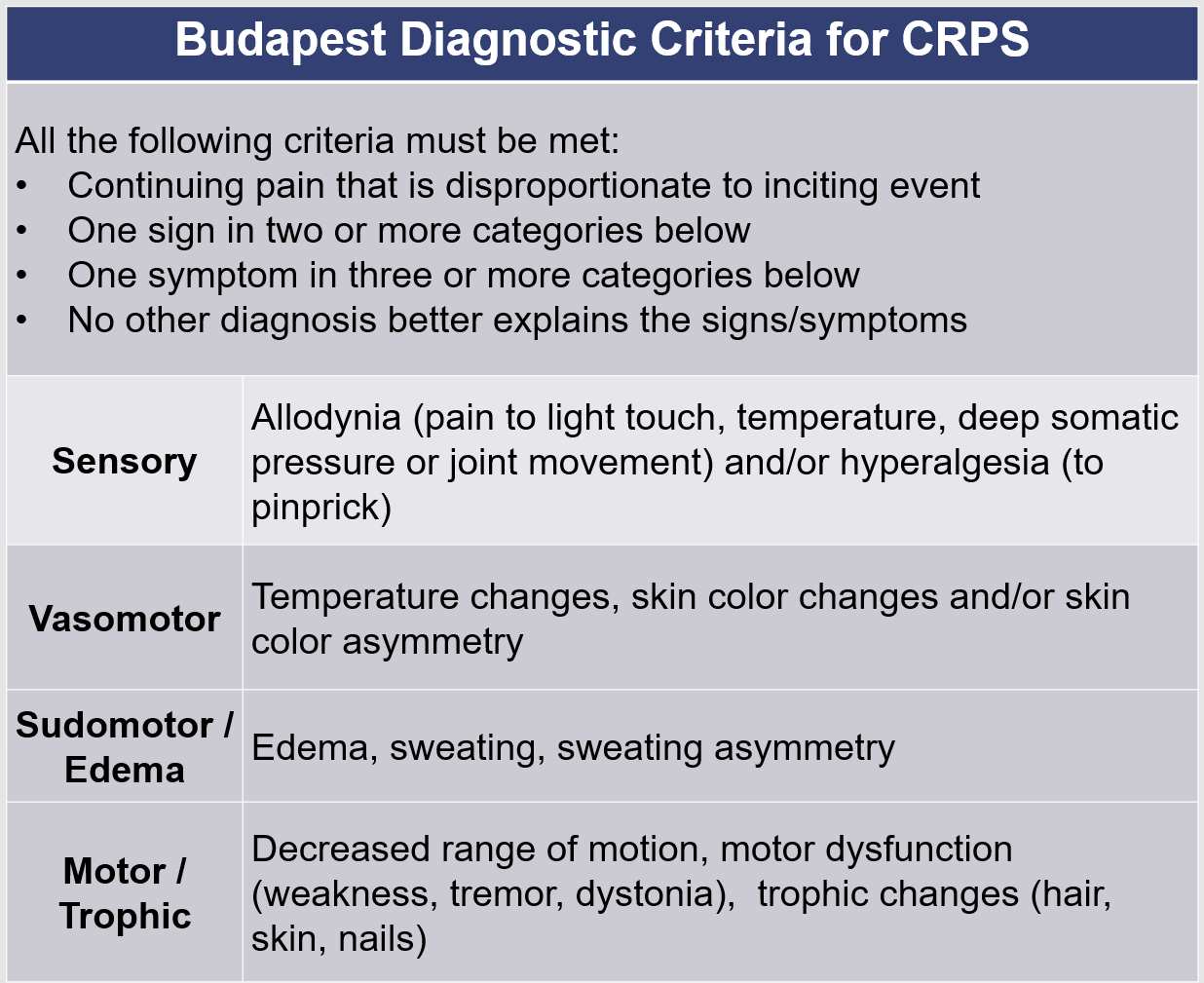
Case Presentation: A 21-year-old woman presented to the emergency department with 1 month of worsening bilateral foot pain, swelling, and erythema. Her symptoms began shortly after a trip to Arizona, where she spent several days hiking and reported use of a strong massage gun on her feet for hours at a time. She was evaluated outpatient by her primary care physician, orthopedic surgery, and urgent care on multiple occasions and treated with amoxicillin, ketorolac, prednisone, diclofenac, ibuprofen, and meloxicam without a definitive diagnosis or improvement. By the date of admission, her foot pain was intractable, and only relieved through prolonged submersion in cold-water baths. The initial differential diagnosis Included an atypical presentation of reactive or autoimmune arthritis, cellulitis or soft tissue infection, erythromelalgia, Complex Regional Pain Syndrome (CRPS), cold-related soft tissue injury (related to the baths) and vascular or venous injury. She underwent extensive vascular, rheumatological, infectious and neurological workup. Notable normal testing included MRI and doppler ultrasound, ESR/CRP, ANA, Rheumatoid Factor, Creatine Kinase, ANCA, Uric Acid, and Antistreptolysin O. Bilateral popliteal nerve blocks provided relief of her foot pain and resolution of the swelling and erythema. She met the Budapest criteria for diagnosis of CRPS, which was suspected due to the negative workup. She was enrolled in comprehensive rehabilitation after evaluation by PM&R which led to partial pain remission. She then underwent a lumbar sympathetic nerve chain block followed by ablation with marked improvement in her pain.
Discussion: CRPS is a musculoskeletal pain syndrome characterized by severe distal limb pain that classically develops following trauma and is disproportionate to the inciting event. Fracture is a common trigger, but CRPS can also develop with benign triggers such as IV placement or without an identifiable trigger at all. Pediatric patients more commonly present with minimal to no trauma prior to the onset of CRPS and more frequently have involvement of the lower extremities as compared to adults. Stress is thought to play an important role in the development of CRPS and there is a high prevalence of preexisting anxiety and depression in pediatric CRPS patients. Early involvement in a comprehensive multidisciplinary treatment program has been shown to improve multiple outcome metrics for CRPS patients, such as improved physical functioning and increased use of positive coping strategies. Interventional pain control techniques such as lumbar sympathetic blocks have limited and conflicting evidence, but have been shown to be effective in some cases of refractory CRPS.
Conclusions: The potential for a seemingly benign stimulus to trigger a severe pain syndrome can make diagnosis of CRPS challenging without a high degree of suspicion. CRPS can also be easily confused with other common conditions such as cellulitis, which can lead to significant delays in diagnosis and appropriate treatment. Common analgesics like opiates are shown to be ineffective in treatment of CRPS. As such, early utilization of multi-modal pain control tailored to CRPS along with early involvement in a comprehensive rehabilitation program is crucial to the effective long-term management of CRPS. The use of interventional pain control techniques should also be considered in refractory cases. While rare, prompt recognition of CRPS and differentiation from its mimics can help lead to improved patient outcomes.