Background: The Surviving Sepsis Campaign strongly recommends that all hospitals screen for sepsis as part of performance improvement. The effect of screening for sepsis on mortality, length of stay, and time to antibiotics is uncertain.
Methods: A systematic literature search was conducted using Cochrane Library, Google Scholar, Ovid Embase, Ovid Medline, Scopus, and Web of Science Core Collection from earliest entry to June 1, 2024. We included all randomized controlled studies of any type of alert system to screen adult patients for sepsis. Risk of bias was assessed using the Cochrane Risk of Bias Tool. Outcomes were pooled using random effects meta-analysis. Strength of evidence was rated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system.
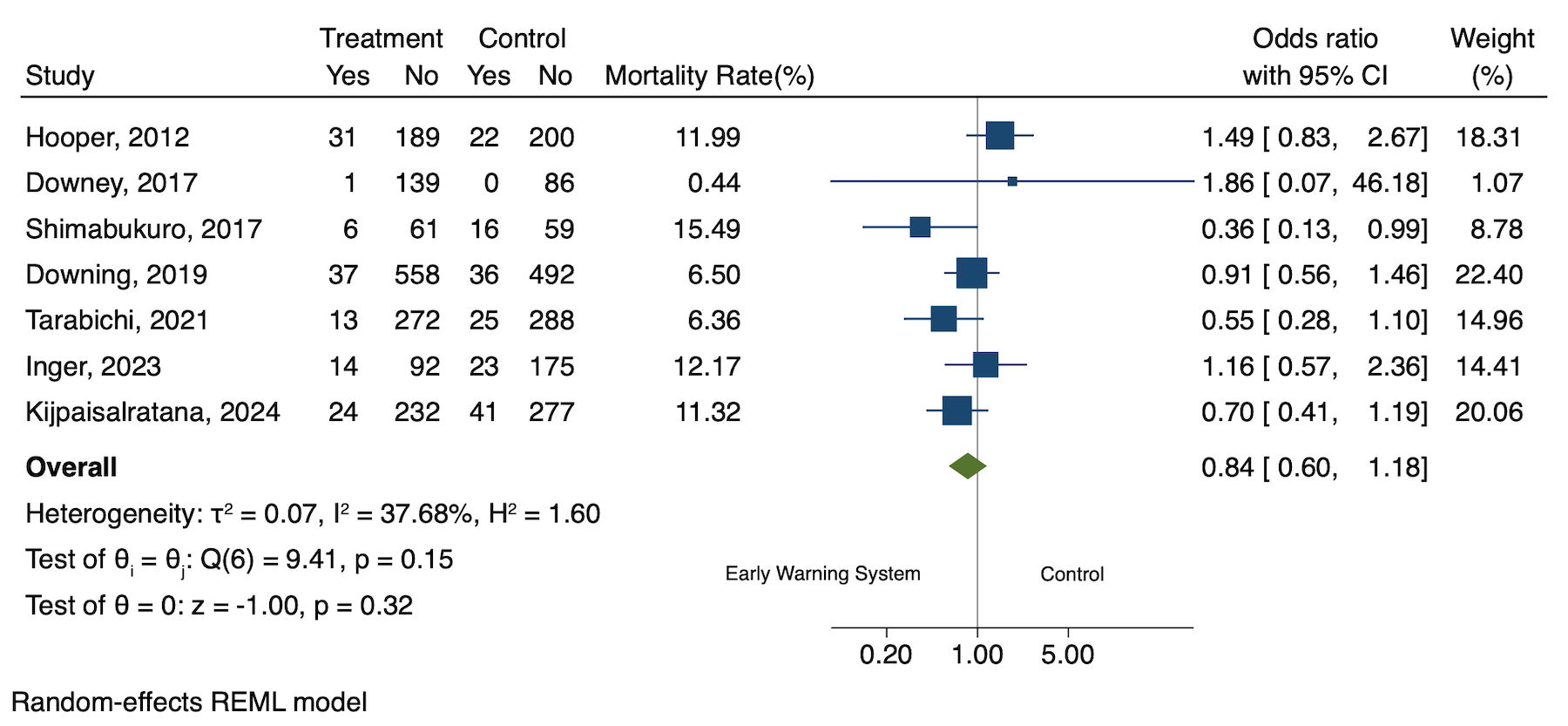
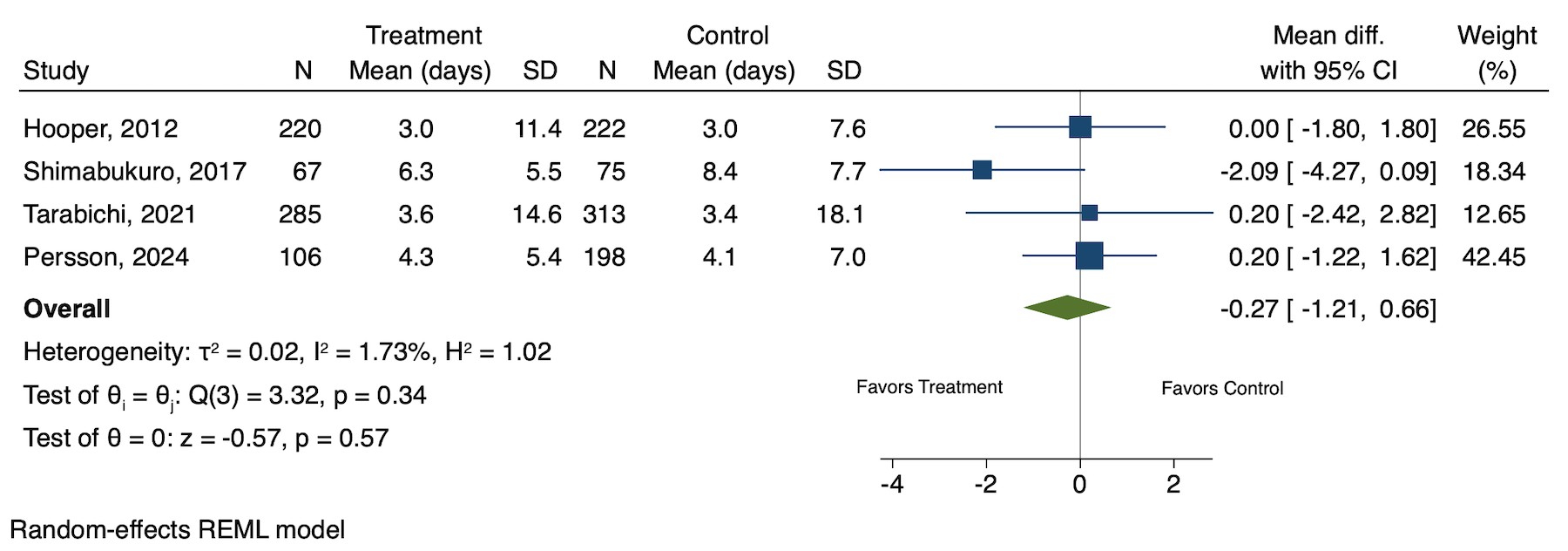
Results: In total, we found 7 studies of 3409 patients with sepsis. The pooled odds ratio for mortality for patients randomized to early warning systems was 0.84 (95% CI, 0.60, 1.18). The average time to antibiotics was reported in 4 studies and found to be 0.08 hours faster in the screening group (95% CI, -0.44, 0.28). Length of stay was reported in 4 studies and found to be 0.27 days less in the screening group (95%, -1.21, 0.66). All differences were non-significant. Overall strength of evidence was low due to risk of bias and imprecision.
Conclusions: Based on the current body of randomized controlled studies, there is no evidence that early screening for sepsis improves outcomes. Guidelines should reconsider current recommendations for screening for sepsis.