Background: The Center for Medicare and Medicaid Services (CMS) instituted the Readmissions Reduction Program to incentivize improvements in care transitions for patients with several common and serious illnesses, including heart failure, acute myocardial infarction, pneumonia, and more recently COPD exacerbations. The HOSPITAL score has been shown to accurately identify medical patients at high-risk for 30-day potentially avoidable readmission, but has never been validated specifically for the medical diagnoses targeted by CMS. We aimed to assess whether the HOSPITAL score would perform well specifically in patients with the primary CMS conditions listed above.
Methods: We retrospectively included all consecutively discharged patients from 6 US hospitals between January and December, 2011. We excluded patients who died before discharge or who were transferred to another acute care facility. The primary outcome was any 30-day readmission that was classified as potentially avoidable using the previously validated SQLape algorithm. By comparing ICD-9 diagnosis codes from the two hospitalizations, SQLape excludes foreseen readmissions such as chemotherapy and readmissions for new diseases unknown during the preceding hospital stay unless a complication of care. The performance of the HOSPITAL score was evaluated according to its overall accuracy (Brier score), its discrimination (C-statistic, representing the area under the ROC curve) and its calibration (based on the Pearson goodness-of-fit statistic).
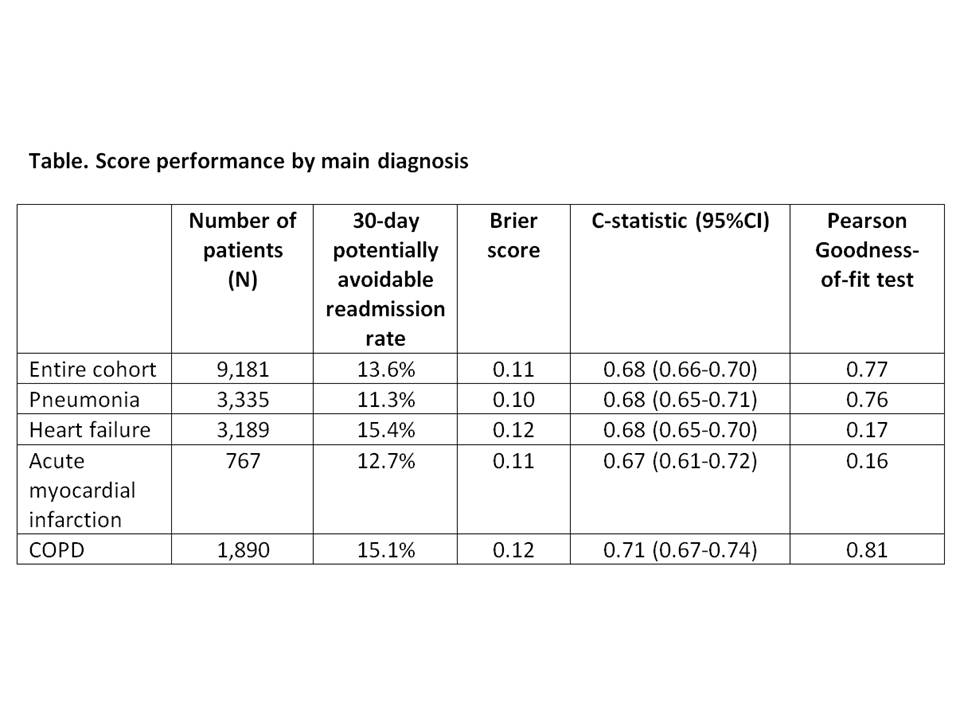
Results: During the study period, 9,181 patients were discharged with a main diagnosis of pneumonia (n=3,335, 36.3%), heart failure (n=3,189, 34.7%), acute myocardial infarction (n=767, 8.4%), or COPD (n=1,890, 20.6%). Overall, the 30-day potentially avoidable readmission rate was 13.6%, and the HOSPITAL score had a Brier score of 0.11 (indicating very good accuracy) and a C-statistic of 0.68 (95%CI 0.66-0.70) in the entre cohort, indicating fair to good discrimination. The Pearson goodness-of-fit test showed a p value of 0.77, indicating very good calibration. The accuracy and the calibration were good for all 4 diagnoses tested, although calibration seemed to be higher for pneumonia and COPD than for acute myocardial infarction or heart failure. In terms of discriminatory power, the C-statistic ranged from 0.67 to 0.71 for each of the diagnoses (table).
Conclusions: The HOSPITAL score performed well in identifying 30-day potentially avoidable readmission in patients hospitalized with a main diagnosis of pneumonia, heart failure, acute myocardial infarction, and COPD. This score has the potential to easily identify patients in need of more intensive transitional care interventions when hospitalized for one of these main diagnoses.