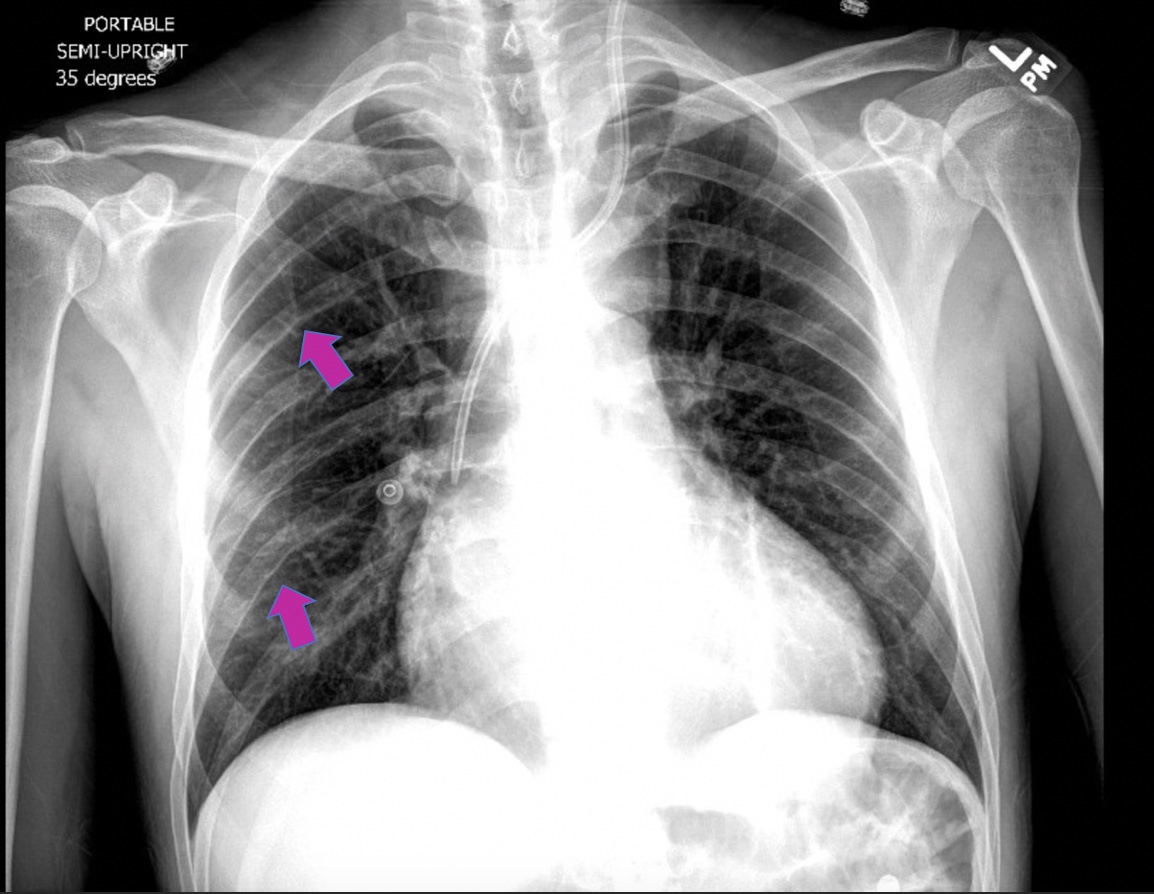
Case Presentation: A 44-year-old man with bicuspid aortic valve and atrial flutter was admitted to the hospital with dyspnea and found to have cardiogenic shock with rapid atrial fibrillation. He received inotropic agents, afterload reducing agents, and cardiac resynchronization therapy, resulting in improvement in symptoms and systolic function. Physical examination demonstrated vigorous carotid pulsations, known as Corrigan’s pulse and alternating flushing and blanching of the nail bed in concert with the cardiac cycle, known as Quincke’s pulse. These findings are classically associated with aortic insufficiency. However, echocardiography demonstrated mild aortic regurgitation, not severe enough to explain the physical findings. Evaluation of the peripheral pulses revealed radial-femoral delay and a 30 mm Hg difference between the systolic blood pressures in the upper and lower extremities. Chest x-ray showed rib notching (Roesler’s sign). These findings were consistent with aortic coarctation. Despite being a congenital anomaly, aortic coarctation can present in adulthood and should be considered in patients with Corrigan’s pulse or Quincke’s pulse. This patient was discharged from the hospital with referral to adult congenital cardiology for further management.
Discussion: Corrigan’s pulse and Quincke’s pulse are commonly seen in patients with chronic, severe aortic regurgitation, and occur when a large systolic stroke volume (from increased preload) is followed by a rapid diastolic collapse in arterial pressure (from backflow of blood into the left ventricle)1,2. These physical findings are also seen in coarctation of the aorta, in which there is high blood flow and pressure proximal to the narrowed segment of the aorta, giving rise to vigorous peripheral pulses in the associated distribution3. To our knowledge, this is the first time Quincke’s pulse has been reported in a patient with coarctation of the aorta. Rib notching develops over time due to the erosions of the bone caused by increased blood flow and pressure through dilated intercostal arteries that have developed to supply collateral flow to the post-coarctation segment of the aorta4
Conclusions: Physical examination skills remain an essential part of a patient’s evaluation and should lead clinical decision making for Hospitalists.