Case Presentation: We present the case of a 59-year-old African American female with no past medical history who presented with 6 weeks of progressively worsening fatigue, weakness, poor oral intake, and noticeable unintentional weight loss. Physical exam revealed 3 out of 5 muscle strength of all extremities and hyperpigmentation of the hands and feet bilaterally. Initial lab findings were significant for pancytopenia and macrocytic anemia. Further evaluation of her pancytopenia included a high LDH , low haptoglobin, high CRP, and a very low vitamin B12 level. A subsequent MRI of the thoracic and cervical spine demonstrated hyperintensity of the dorsal columns consistent with demyelination likely secondary to subacute combined degeneration. Despite an negative intrinsic factor antibody test, the diagnosis of pernicious anemia was eventually confirmed with a positive antiparietal cell antibody test. After a week of daily subcutaneous B12 injections, significant improvement in reticulocyte, ANC, WBC, and platelet count was noted.
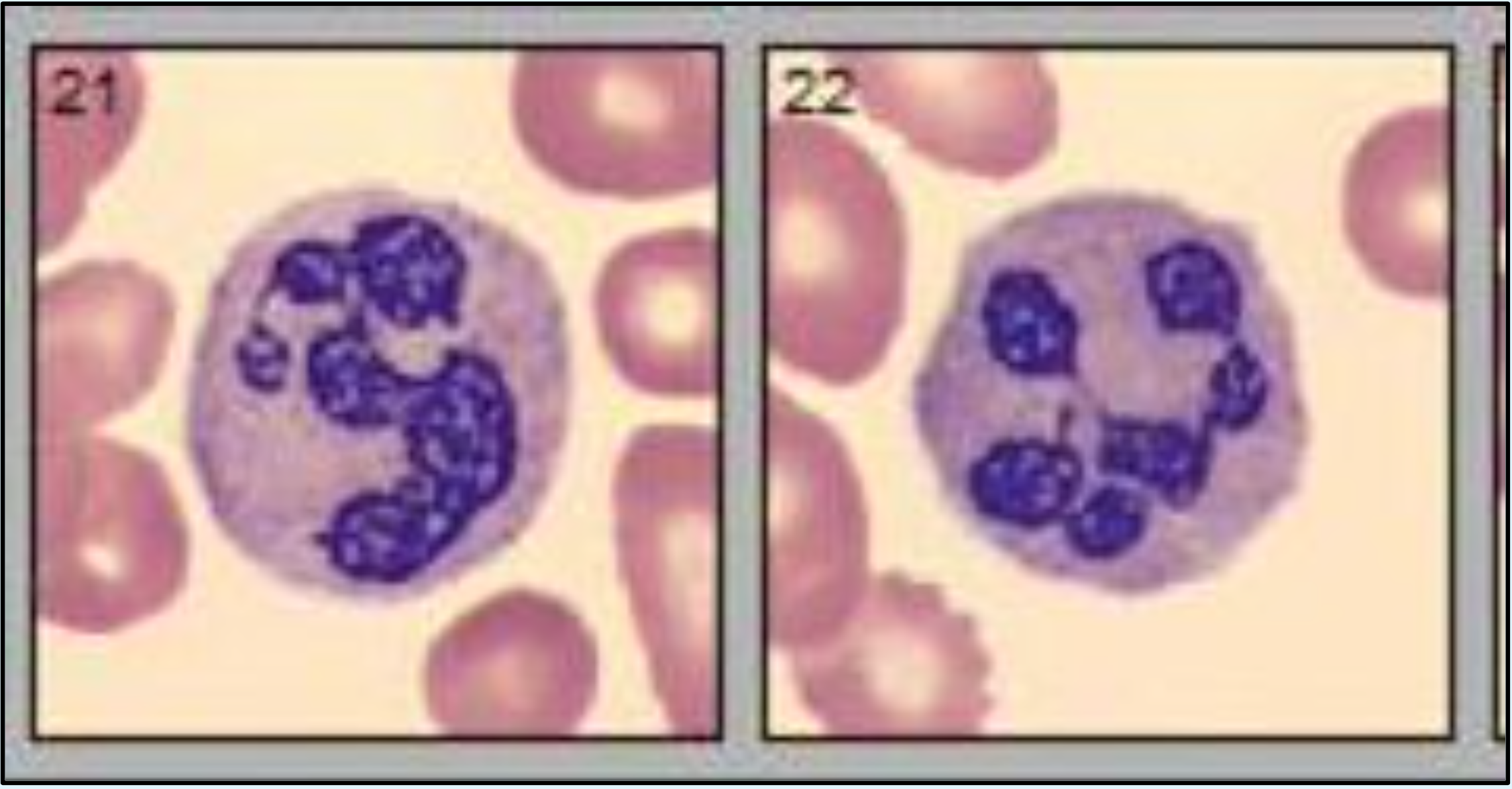
Discussion: This case underscores the critical importance of timely recognition and treatment of vitamin B12 deficiency, particularly in the context of pernicious anemia. Vitamin B12 deficiency, due to its essential role in DNA methylation and nucleotide synthesis, can present with a broad spectrum of clinical manifestations, ranging from hematological to neurological deficits. Hematologically, the deficiency often manifests as megaloblastic anemia, but can also lead to more severe conditions such as hemolysis and, in rare cases, pancytopenia. The complexity of these presentations can complicate diagnosis, as they may mimic other serious conditions such as myelodysplastic syndromes (MDS), acute leukemia, and thrombotic thrombocytopenic purpura (TTP). In this case, the patient presented with pancytopenia, hypersegmented neutrophils, and neurological symptoms indicative of subacute combined degeneration (SCD) of the spinal cord. These findings highlight the diverse manifestations of severe B12 deficiency and emphasize the necessity for a thorough differential diagnosis that includes both hematological and neurological etiologies. The presence of hyperpigmentation on the palms and soles, though not always recognized as a classic sign of B12 deficiency, further complicated the clinical picture, illustrating the condition’s potential to mimic other diseases. Prompt investigation of the underlying cause of B12 deficiency is crucial, as it directly influences the treatment approach. For patients diagnosed with pernicious anemia, as in this case, daily subcutaneous or intramuscular injections of B12 are essential to prevent permanent neurological damage.
Conclusions: This case is important because it demonstrates the diverse and severe manifestations of Vitamin B12 deficiency, which can masquerade as other hematological conditions, complicating diagnosis. Understanding these presentations ensures timely intervention, preventing irreversible neurological damage and improving patient outcomes through appropriate management strategies. This case emphasizes the necessity of rapid B12 repletion to prevent permanent neurological damage, stressing the importance of timely intervention even in the absence of classical diagnostic markers. Clinicians must maintain a high index of suspicion for B12 deficiency in patients with unexplained anemia and neurological symptoms.