Background: Emory Healthcare’s approach to monitoring high-risk mortality patients relies heavily on retrospective data collection and analysis, which delays identification of and addressing critical issues. Additionally, the absence of standardized processes for mortality reviews and improvement efforts across the system leads to inconsistent practices and hinders proactive quality improvement initiatives.
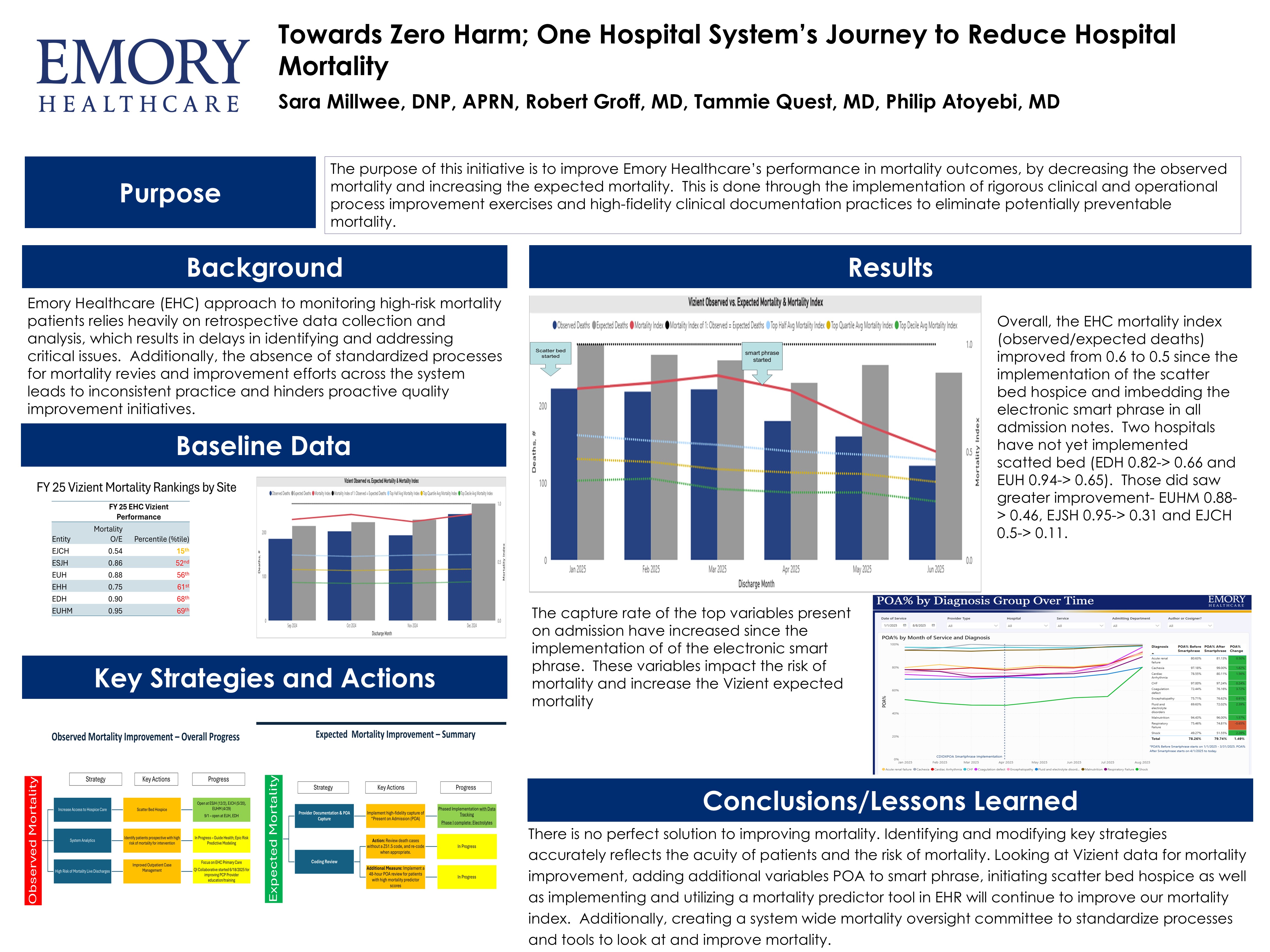
Purpose: We seek to improve Emory Healthcare’s (EHC) mortality index and outcomes by decreasing misclassified observed mortality and increasing expected mortality. This is done with a two-pronged approach: utilization of scatter bed hospice (where patients receive hospice care in situ without disruption or hospice bed limitations, and are appropriately removed from observed mortality metrics) and an electronic health record (EHR) smart phrase.
Description: We implemented scatter bed hospice and an intuitive smart phrase in the EHR. Scatter bed hospice allows hospice patients, at end of life, to die in hospice care. The EHR tool helps capture variables and conditions that are present on admission to the hospital, which accurately impact the acuity and complexity of our patients.
Conclusions: The overall mortality index decreased to 0.5 in June 2025 (observed deaths=113; expected deaths=227.54). Scatter bed hospice was gradually rolled out to different hospitals and the EHR smart phrase was embedded into all admission notes. Additionally, an EHC Mortality Oversight Committee was established to ensure robust, standardized, and sustainable mortality oversight that drives continuous learning, enhances patients’ quality of care, and positions EHC within the top quartile of Vizient ranking. While there is no perfect solution to improving mortality. Initiating scatter bed hospice and developing a EHR tool to help capture variables present on admission have demonstrated improvement to our mortality index. We are continuously evaluating how to add to and improve these strategies.