Background: Transition of care, particularly at the point of discharge, is a pivotal part of the patient’s healthcare journey, carrying substantial risks to safety and quality of care. Whether a patient is discharged to home, an outpatient rehabilitation center, or a skilled nursing facility, each transition introduces opportunities for errors. Errors may include inaccurate medication reconciliation, incomplete or vague follow-up instructions for managing medical devices such as wound vacs or feeding tubes, and insufficient guidance for post-hospitalization provider follow-up. When these processes are inadequately managed, patient outcomes can suffer, hospital readmissions may increase, and medicolegal risks for providers can rise. Ensuring that follow-up appointments with care providers are timely and well-coordinated is essential for seamless continuity of care. Gaps in these transition processes can lead to adverse clinical events, decreased patient satisfaction, and contribute to preventable readmissions.
Purpose: Anecdotal reports identified several instances where key discharge steps were missed: essential medications left unprescribed, missing instructions for postoperative drains, and unscheduled follow-up appointments. These lapses occasionally resulted in unplanned readmissions. Recognizing this, the Chief Nursing Officer and Chief Medical Officer proposed a standardized discharge checklist to bring consistency to the discharge process, enable real-time error correction, and reduce avoidable readmissions.
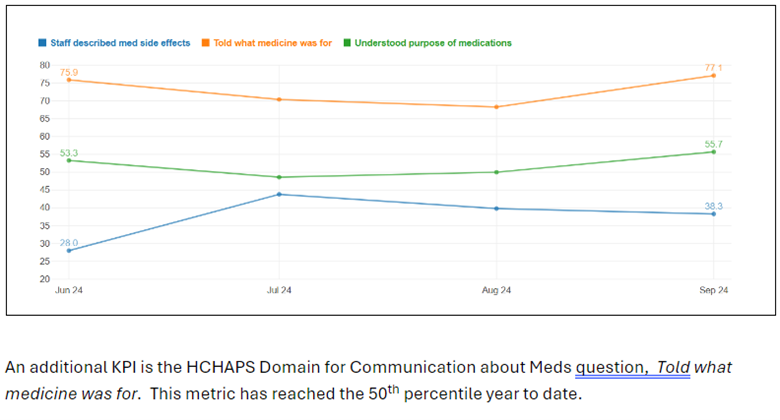
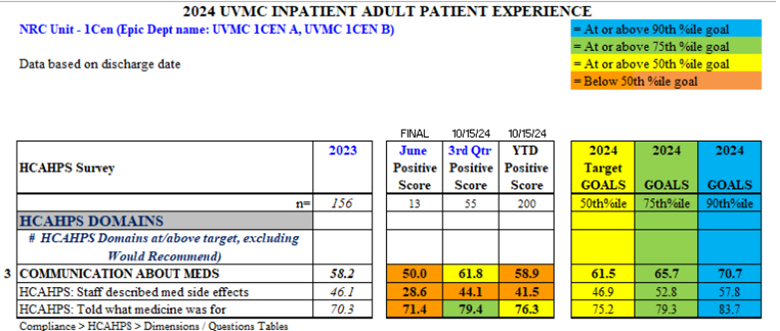
Description: Developed collaboratively by the unit manager, associate nurse manager, and bedside staff, the discharge checklist covers key areas, including disease management education, postoperative care instructions, discharge medication accuracy (including home medications), medication education, and identifying home-care needs. Staff received training, and the checklist trial was launched and monitored weekly for compliance by unit leadership. Key performance metrics were based on Patient Experience data, using HCAHPS and NRC Health’s Real-Time Feedback Management data, which measure the percent of positive responses (9 or 10 on a 10-point Likert scale) to a given patient experience question.Additional NRC Real-Time questions relevant to discharge were added to track the impact on the pilot unit. Anecdotally, the checklist corrected critical oversights, such as missed medications and missed drain care instructions, preventing possible adverse events.
Conclusions: The pilot findings indicate that the checklist improved discharge medication accuracy, facilitated in-hospital prescription fills, and allowed customized follow-up scheduling to suit patient availability. Positive trends in HCAHPS and NRC Real-Time questions related to medication instructions have emerged. Given these promising results, the discharge checklist will be implemented across other inpatient units. We anticipate further reductions in readmissions and enhanced patient experience metrics as the innovation scales.