
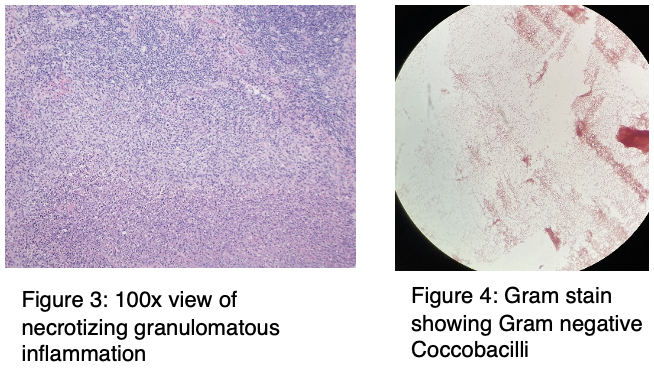
Case Presentation: A 28-year-old male who was immunosuppressed with Infliximab for Crohn’s disease was seen in the hospital in early summer for non-resolving fever of four-week duration. Blood and urine cultures and computed tomographic (CT) imaging of chest, abdomen and pelvis was negative along with molecular testing for common tick-borne diseases like Anaplasmosis, Babesiosis, respiratory pathogens, and pathogens of meningitis. Serological studies for Lyme disease, primary Cytomegalovirus, Epstein-Barr virus and West Nile virus infections were also negative. The patient received empirical antibiotics and prednisone without resolution of fever. A week after his presentation, he developed a sore throat and was found to have cervical lymphadenopathy. CT scan of his neck revealed the presence of necrotizing lymphadenopathy. An open lymph node biopsy was performed. Pathological analysis of the tissue revealed presence of extensive necrotizing granulomas. Cultures of the lymph node tissue grew gram negative coccobacilli, which were ultimately identified as Francisella tularensis. A serological testing performed for tularemia was also reported to be positive for both IgM and IgG antibodies. The patient was treated with a two-week course of ciprofloxacin and doxycycline which led to complete symptom resolution. The patient did not recall any tick bites, but he had extensive outdoor exposure related to his employment as a manager of a local golf course.
Discussion: Tularemia cases are relatively rare throughout most of the United States. Exposure occurs primarily through tick bite, handling of infected animals, or inhalation of aerosols contaminated with Francisella tularensis. This patient was likely exposed to an infected animal or had an unknown tick exposure. Our patient had the glandular form of Tularemia, the third most common syndrome among adults after ulceroglandular and oropharyngeal forms. Due to the rare nature of Tularemia, its variability in symptoms and lack of robust randomized clinical trial data treatment recommendations are based on expert consensus and there are significant variations in practice. A literature review suggests that outcomes might be better with quinolones as compared to aminoglycosides and tetracyclines. In some cases, combination therapy may be required. Our patient was treated with doxycycline and ciprofloxacin which led to complete resolution of symptoms.
Conclusions: Diagnosis of Tularemia can be difficult to establish due to its varying symptomatology and rarity, especially outside of endemic areas. Illness can be particularly severe and disabling, particularly in immunocompromised patients. Diagnosis requires a high index of suspicion and may occasionally require invasive procedures, like a biopsy, as was the case in this patient. Once diagnosed, treatment usually consists of mono or combination therapy based on severity of illness and the patient’s underlying medical conditions. However, creating evidence-based treatment guidelines to standardize practice will require further research.
.png)