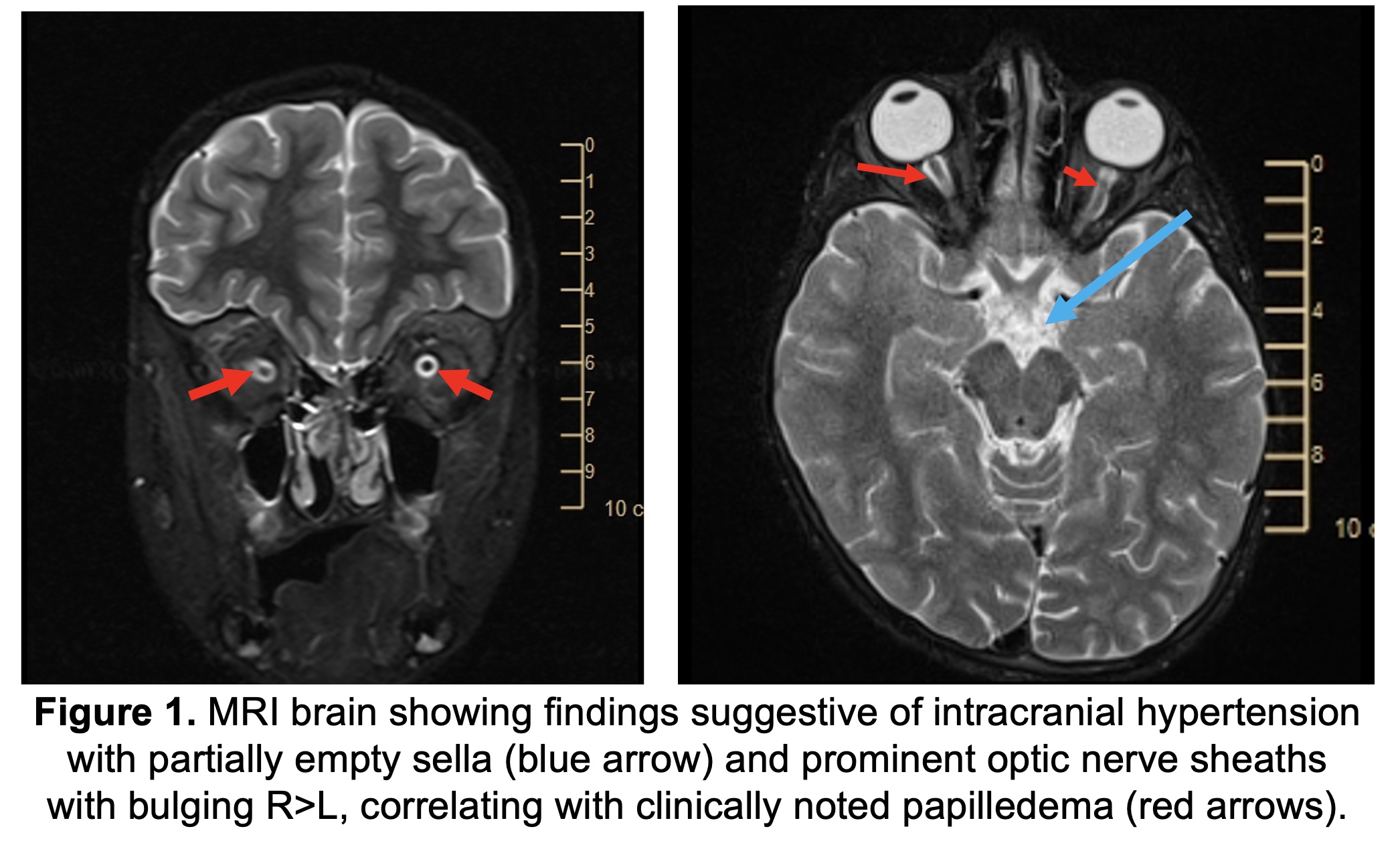
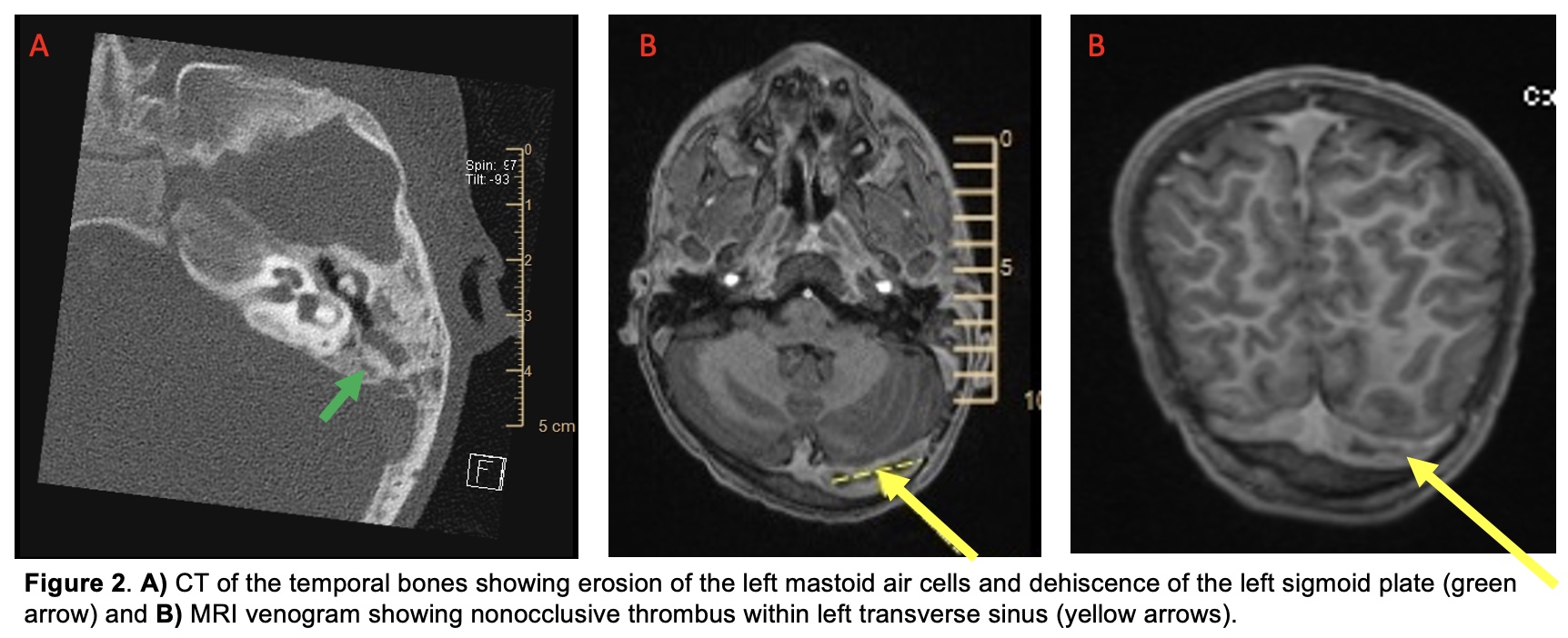
Case Presentation: A 7 year-old with hypohidrotic ectodermal dysplasia (ED) and recurrent sinusitis was admitted with diplopia, headaches, and fevers. In the preceding 2 months, he had multiple episodes of fever, nasal impetigo, and positive group A strep (GAS) throat swabs without pharyngitis. He was treated twice with azithromycin due to allergies to amoxicillin, cephalosporins, and clindamycin. He had been admitted 5 days earlier for 8 days of fevers and polyarthralgias. An extensive evaluation was unrevealing other than positive rhinovirus and GAS throat culture. He quickly improved and was discharged on azithromycin and intranasal mupirocin for decolonization. Exam was notable for a Tmax of 40.1C, bilateral dense cerumen impaction, nontoxic appearance, and papilledema on fundoscopic exam. Labs revealed leukocytosis, elevated inflammatory markers, and normal CSF studies. Lumbar puncture opening pressure was 30 cm H2O. Brain MRI/MRV demonstrated sinusitis, bilateral mastoid effusions, and non-occlusive left transverse sinus thrombosis. CT showed erosion of the left mastoid air cells and dehiscence of the sigmoid plate. Blood cultures grew Streptococcus pyogenes. He was treated with ceftriaxone, linezolid, heparin, acetazolamide and left myringotomy with drainage of a mucoid effusion. He was discharged on linezolid, rivaroxaban, and acetazolamide after complete resolution of his symptoms. He had no recurrence of fevers after completing antibiotics.
Discussion: This patient’s recurrent fever with impetigo seemed to suggest recurrent GAS infections. He also developed sinusitis and mucoid otitis media, and finally was treated for mastoiditis complicated by sinus venous thrombosis with elevated intracranial pressure and bacteremia. He had improvement with azithromycin, but we suspect his GAS infection persisted and ultimately spread due to inadequate treatment. GAS is increasingly resistant to azithromycin, and the duration would have been inadequate for chronic sinusitis or mastoiditis. It is estimated that 90% of patients who report a history of penicillin allergy can tolerate penicillins, and he tolerated ceftriaxone in the hospital. Our patient has the most common form of ectodermal dysplasia, which is X-linked recessive and characterized by hypotrichosis, hypohidrosis, and hypodontia. These patients are at an increased risk for atopy, respiratory infections, sinusitis, and acute and chronic otitis media. Other rare forms of ED can also be associated with immunodeficiency.
Conclusions: Patients with ectodermal dysplasia benefit from saline rinses, ENT referral, and aggressive treatment of respiratory infections to help prevent potentially serious complications. In a child who has multiple recurrences of GAS infection, it is important to consider predisposing risk factors and inadequate antibiotic treatment (in addition to colonization) as potential explanations. Patients with allergies to beta-lactam antibiotics, especially when predisposed to infection, benefit from proactive referral to an allergist.