Case Presentation: OBJECTIVE- To understand that hypokalemia is common in patients with Duchenne Muscular Dystrophy (DMD) when acutely ill – To understand the mechanism of hypokalemia in patients with Duchenne’s Muscular Dystrophy (DMD)A 62-year-old male with Duchenne Muscular Dystrophy (DMD) who is ventilator-dependent and quadriplegic presented to the hospital with acute onset of fever and constipation. Labs revealed a potassium of 1.7 mmol/L and a magnesium of 2.2 mmol/L. CT scan of the abdomen revealed colitis. The patient was treated with ceftriaxone 1g daily and metronidazole 500mg twice daily for 5 days, with resolution of symptoms. Patient received a total of 500 mEq of potassium over 9 hours with normalization of his hypokalemia. Chart review revealed multiple admissions for pneumonia and an infected sacral ulcer, during which he became hypokalemic and required repletion.
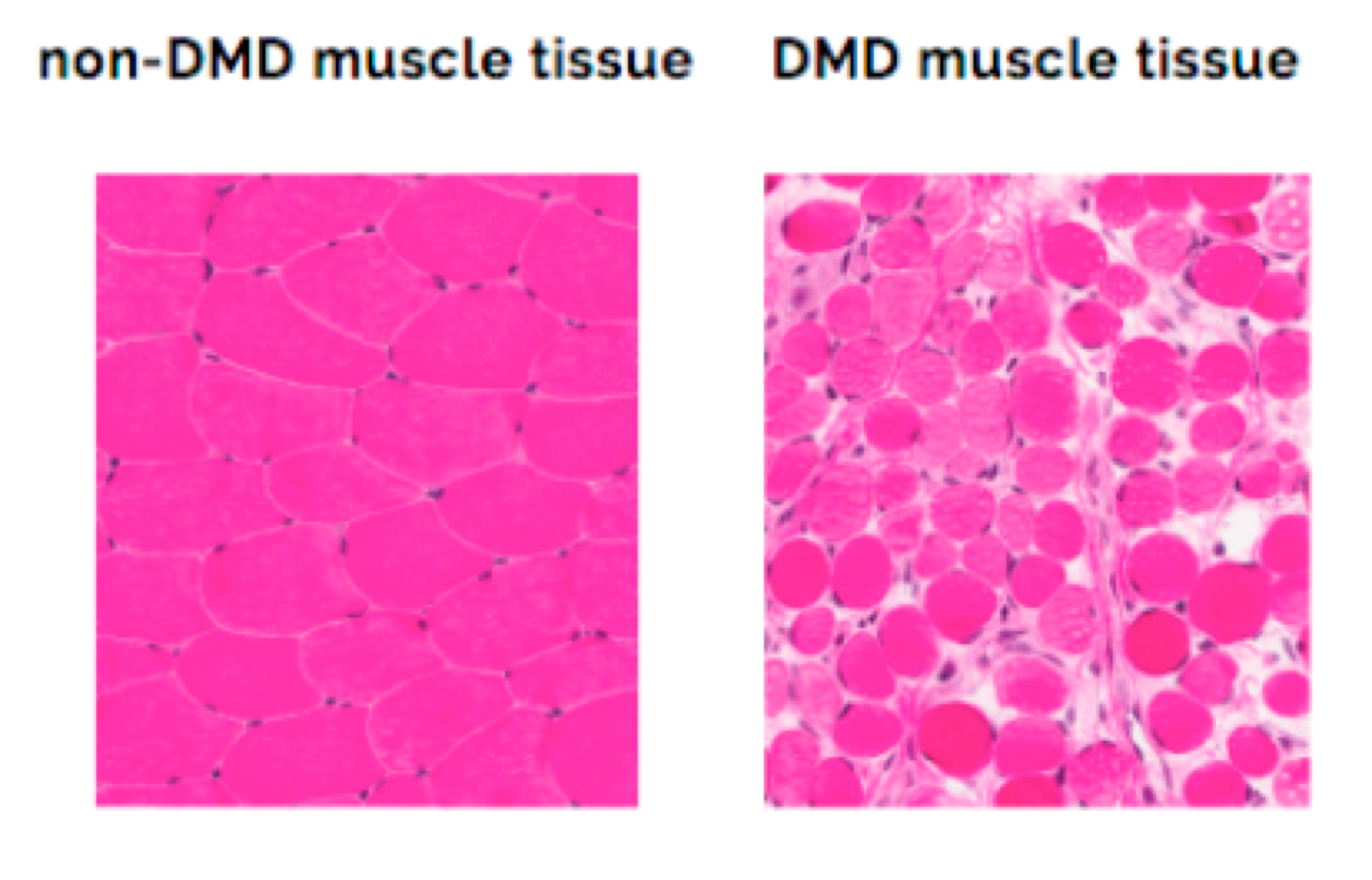
Discussion: DMD is an X-linked recessive disorder in which muscle cells are replaced with connective tissue, leading to musculoskeletal and cardiopulmonary failure. Patients with DMD typically maintain normal serum potassium levels, but have an elevated risk for severe hypokalemia when acutely ill. Hypokalemia arises due to decreased total body potassium stores as a result of the replacement of the potassium-rich muscle cells with collagen and fibers that lack potassium. Severe hypokalemia can result in patients with DMD as a result of relatively minor potassium loss via gastrointestinal or urinary losses, poor oral intake, or via intracellular shift. In addition to pneumonia, this patient had a few episodes of diarrhea after the administration of an enema that was given for constipation prior to arrival. However, the severity of hypokalemia (1.7 mmol/L) was significantly greater than the severity of the overall illness. Previous admissions revealed recurrent hypokalemia even with minor infections. Each time, the patient normalized with repletion within 24 hours. Rapid correction of hypokalemia is possible in this scenario due to the small volume of distribution that needs to be repleted as a result of sarcopenia. Only a few prior cases of patients with DMD and hypokalemia have been reported. Based upon a literature search, this is the oldest patient record with DMD, which is typically cared for in the pediatric setting. With advancing medical care and novel therapies for genetic conditions, it is likely that patients with DMD will live longer and have more hospital encounters with non-pediatric healthcare providers. Providers need to understand the importance of frequent monitoring of potassium levels in patients with DMD when hospitalized with acute illness, as well as the rapidity in which it can be corrected due to the small volume of distribution.
Conclusions: Patients with DMD are at increased risk of severe hypokalemia when acutely ill due to low total body potassium stores. Aggressive repletion can lead to rapid correction due to a low volume of distribution.