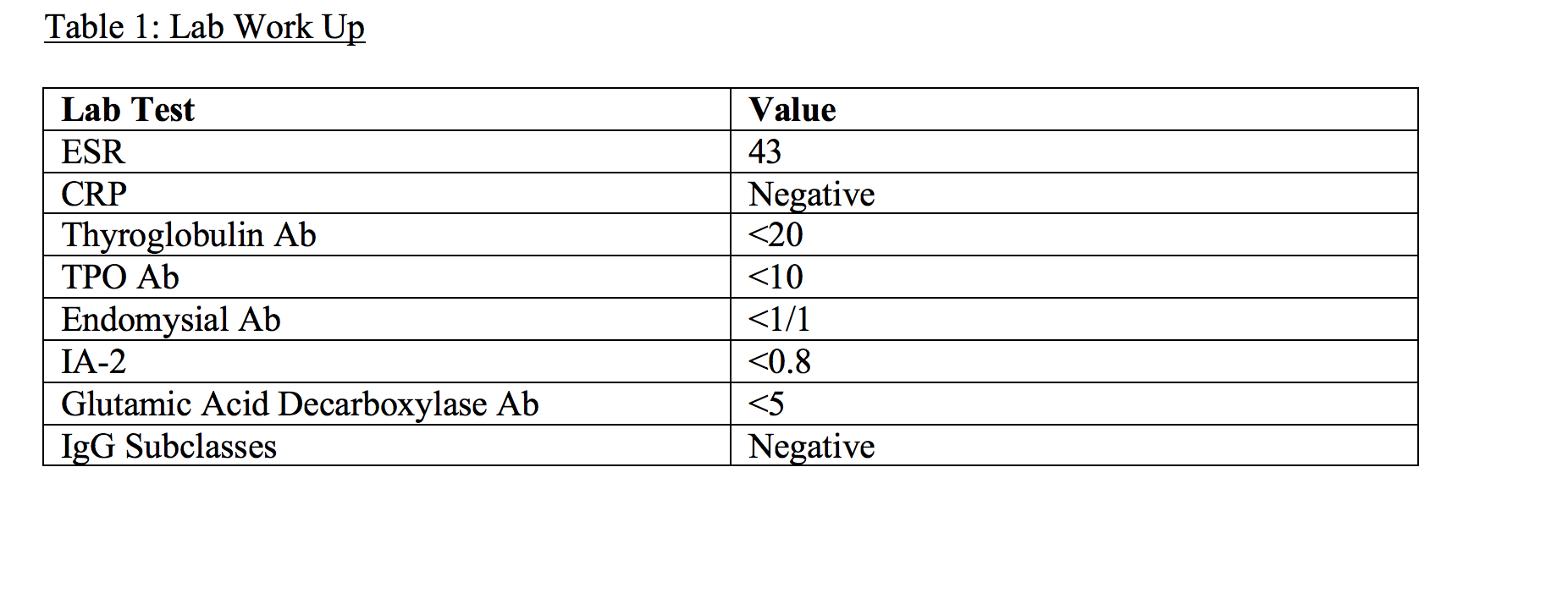
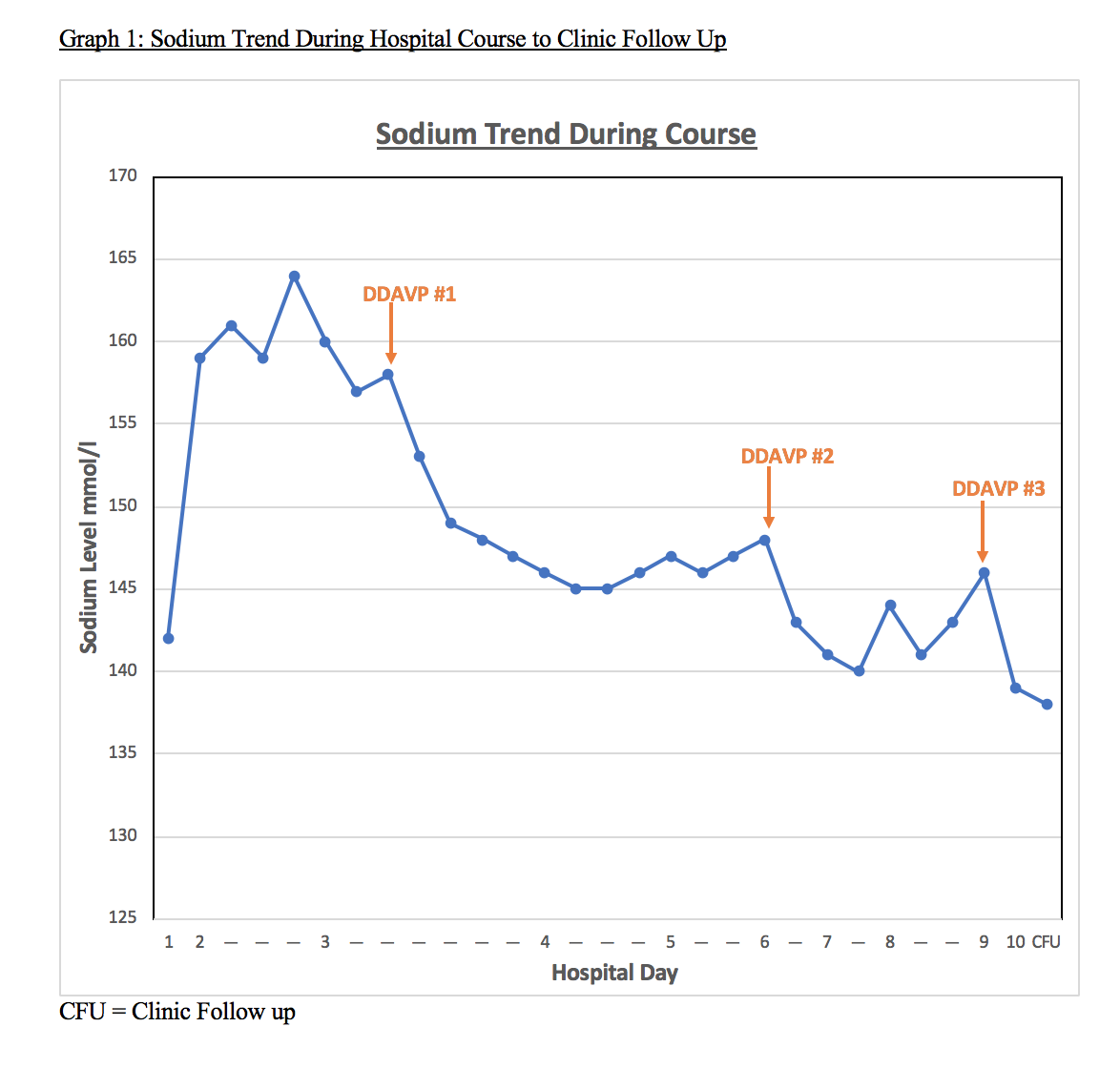
Case Presentation: A 70 year-old woman with no known history was admitted with symptoms of urinary incontinence and generalized weakness. Workup was notable for a positive urinalysis, positive Influenza swab, and serum sodium of 142mmol/L. She was started on ceftriaxone, oseltamivir and isotonic fluids (normal saline). On hospital day (HD) 2, her sodium was 159mmol/L, and she was changed to hypotonic fluid (D5Water). Her respiratory status and mental status acutely declined that day requiring intubation; labs showed a sodium of 164mmol/L. Further testing during this time revealed a high serum osmolality of 340mOsm/kg, low urine osmolality of 87mOsm/kg and low urine sodium of <20mmol/L. Imaging revealed a CT Head without acute infarct and MRI brain with evidence of amyloid angiopathy, however no abnormalities in in the pituitary or hypothalamus. A presumptive diagnosis of Central Diabetes Insipidus (CDI) was made due to the lack of response to hypotonic fluids, and Desmopressin 1mcg (DDAVP) was started on HD 3. A rapid reduction in urine output was observed along with change in serum osmolality to 275mOsm/kg and serum sodium to 141mmol/L. To workup CDI, further labs were obtained, shown in Table 1, none of which revealed an etiology. On HD 5, her mental status improved and she was extubated. Subsequently, due to a rise in sodium to 148mmol/L, increasing urine output and urine osmolality down to 213Osm/kg, she was given a second dose of DDAVP. On HD 9, she received an additional dose of DDAVP due to a rise in sodium level to 146mmol/L. See Graph 1 for trend. She was discharged after the third dose of DDAVP with a serum sodium of 139mmol/L. She was followed up in the clinic after 5 days of discharge with a sodium of 138mmol/L and back to her baseline clinical and mental status.
Discussion: Both acute influenza syndrome and sodium abnormalities are common encounters in the hospital setting. We present a unique case of transient CDI caused by an acute influenza A syndrome, hypothesized to cause a brief reduction in ADH secretion by the pituitary causing a syndrome of acute hypernatremia, hypotonic polyuria and acute encephalopathy. Her CDI had resolved after prompt treatment with oseltamivir and supplementation with DDAVP during the acute viral illness. There has been 1 prior case report of a young man with H1N1 type A virus causing a transient diabetes insipidus.(1) There have been a few postulated mechanisms for this described, including direct viral infiltration of the pituitary seen on MRI(1), although our patient’s did not show evidence of this. In support of a viral etiology in our case, serum blood work for autoimmune conditions that could have caused CDI were negative (Table 1). A viral etiology is most plausible since her sodium levels returned to normal after resolution of her influenza infection.
Conclusions: This is a rarely reported case of CDI in a patient with acute viral syndrome from influenza A. Hospitalists should have a high index of suspicion for CDI in patient with viral illnesses that have persistently elevated sodium levels despite treatment with hypotonic fluids. This should be promptly treated with supportive care, DDAVP and antiviral therapy. In our case, CDI developed rapidly, and it was important for it to be promptly recognized and treated. Finally, it is important to closely follow these patients since the resolution of acute viral illness often obviates the need to continue DDAVP given the transient nature of viral syndromes.