Background: Inpatient hypoglycemia (HG) is common and often avoidable, associated with poor outcomes and high costs, and its prevention reflects hospital performance. We investigated its risk factors and impact on mortality, hospital length of stay (LOS), charges, and readmissions. We defined HG as glucose ≤40 mg/dl (severe), >40 – ≤70 mg/dl (moderate), or euglycemia >70 mg/dl.
Methods: We conducted a retrospective analysis of adults (≥18 y) with diabetes (DM) admitted to a quaternary center using electronic health record data extracted through a business intelligence tool and compared HG vs. euglycemia. HG was the primary outcome predictor in multivariable models adjusted for covariates, including severity of illness (SOI). The analysis encompassed 54,502 unique admissions of patients with type 1 (7.2%) or type 2 (92.8%) DM across medical (66.8%), surgical (30.3%), and other services (2.9%) in intensive care units (ICU) (7.3%) and non-ICU settings (92.7%) over a 10-year period. Among these patients, 9,903 (18.2%) experienced at least one moderate (M) HG episode, while 1,535 (2.8%) had at least one severe (S) HG episode.
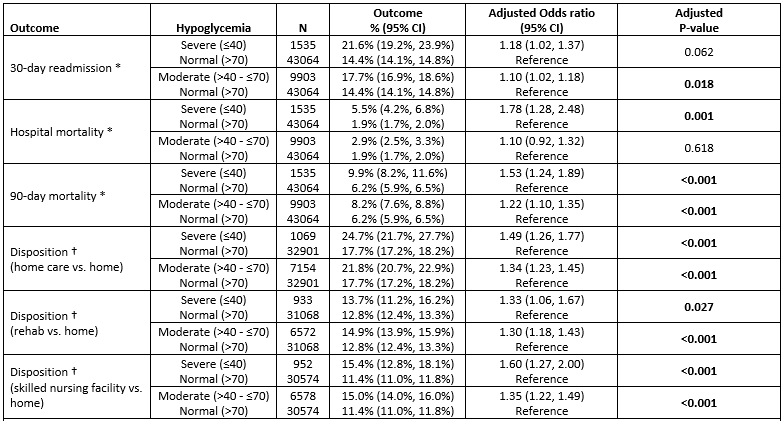
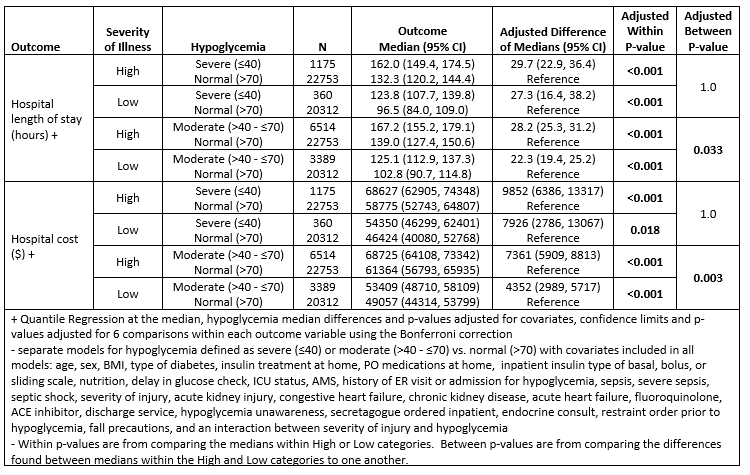
Results: Factors significantly associated with either M or S HG in the hospital included type 1 DM (P< 0.001), preadmission insulin use (P< 0.001), receiving insulin in the hospital (P< 0.001), fasting status (S P=0.002), enteral or parenteral nutrition (P< 0.001), restraints orders (S P=0.022, M P< 0.001), first point-of-care glucose >12 hours from admission (P< 0.001), ICU status (P< 0.001), high SOI (P< 0.001), altered mental status (P< 0.001), prior admission for HG (P< 0.001), sepsis, acute and chronic kidney injury, HG unawareness (P< 0.001), chronic congestive heart failure (HF) (S P=0.037, M P< 0.001), acute HF (S P=0.034, M P< 0.001), fall risk (M P< 0.001), and chronic liver disease (M P=0.008). Outcomes analysis revealed that S HG was associated with in-hospital mortality (P=0.001). M HG was associated with 30-day readmission (P=0.018). Both M and S HG were associated with 90-day mortality (S P< 0.001, M P< 0.001), post-discharge home care (S P< 0.001, M P< 0.001), rehabilitation facility (S P=0.027, M P< 0.001), or skilled nursing facility care (S P< 0.001, M P< 0.001), all statistically independent from SOI. M and S HG increased median LOS (P< 0.001) and median hospital charges (P< 0.001) among severely and non-severely ill subjects. The increases were more pronounced in the high-SOI group for M HG (P=0.033, P=0.003), but not for S HG (P=1.0, P=1.0).
Conclusions: HG’s impact extends beyond being a mere illness marker, suggesting danger regardless of SOI. Predisposing factors can be anticipated in clinical practice, underscoring the need for preventive measures and individualized assessments. It may be relevant to categorize hypoglycemia as mild (56-70 mg/dl), moderate (40-55 mg/dl), and severe (< 40 mg/dl) to better understand its effects on outcomes, and consider other risk factors to improve prevention strategies, enhance patient care and optimize hospital resources.