Background: The Antinuclear Antibody test (ANA) is a test often positive in patients with autoimmune rheumatologic disorders. However, ANA testing can also be positive in non-rheumatic conditions and in healthy individuals1. Prior studies have focused on the clinical utility of positive ANA testing in the outpatient setting by non-rheumatologists, but less is known about its utility in the inpatient settings2. ANA testing can easily be ordered for hospitalized patients, but when positive may require rheumatology consultation to determine if a rheumatic disorder (RD) is present. We evaluated whether a positive ANA test in hospitalized patients and subsequent rheumatology consultation resulted in a new diagnosis of RD.
Methods: We reviewed our institution’s hospital admissions from January 2017 to January 2020 for patients aged 18-80 years old with a rheumatology consultation for a positive ANA (titer>1:160). Data collected included patient demographics (age, sex, and race/ethnicity as reported in the electronic health record), ordering team, comorbidities, rheumatologic history, other autoimmune disease history, other positive serologies, context ANA ordered, and subsequent diagnosis of a RD.
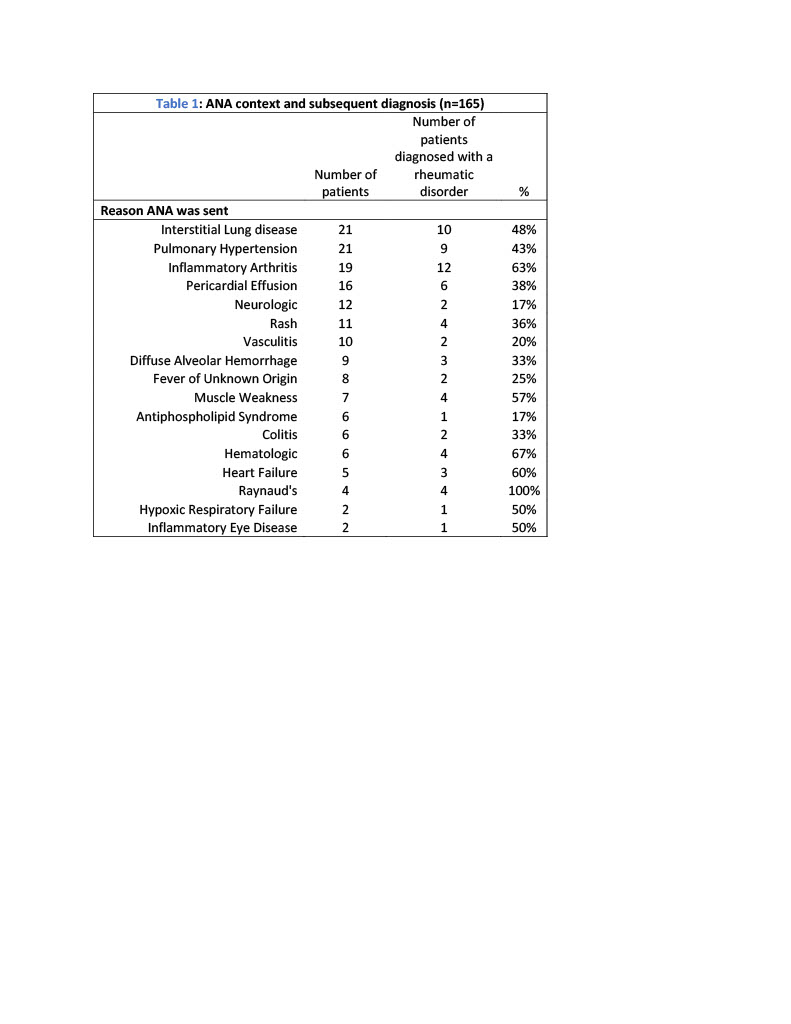
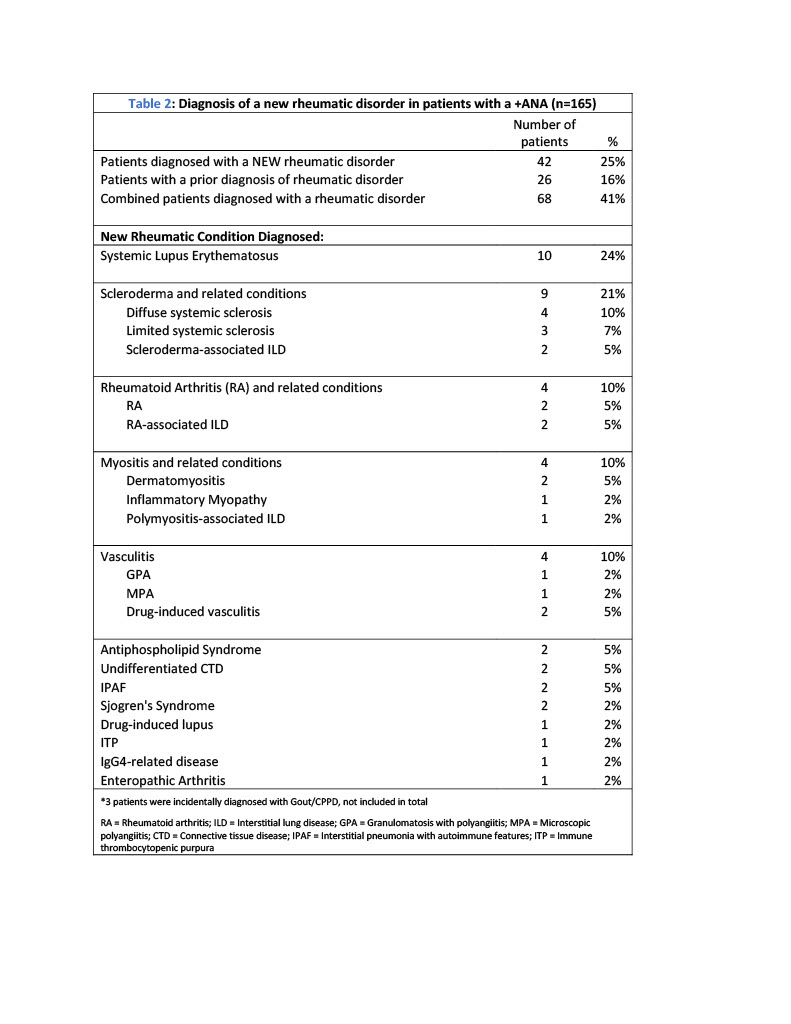
Results: Baseline characteristics of 165 patients were analyzed (Table 1). The most common contexts for ordering ANA were interstitial lung disease (ILD), pulmonary hypertension (PH), and inflammatory arthritis (Table 2). 41% of all patients with a positive ANA were diagnosed with RD: 25% were newly diagnosed with RD after rheumatology consultation and 16% were noted to have a prior RD diagnosis (Table 3). The most frequent new RD was Systemic Lupus Erythematosus (SLE) (24%) followed by Systemic Sclerosis (SSc) (21%). RD was diagnosed in 40-50% of patients with ILD or PH, and 63% of patients with inflammatory arthritis.
Conclusions: In our study of hospitalized patients, only 25% of those with a positive ANA were newly diagnosed with RD. ANA testing was often used despite previous results being known or to confirm diagnosis of an established RD. Our study was not designed to detect differences between likelihood of RD in different clinical settings, but given their frequency, inpatient ANA testing may be most useful in evaluation of suspected SLE and SSc. ILD and PH were common reasons for ANA testing, likely related to our institution’s robust heart and lung programs. ANA testing resulted in RD diagnosis in 40-50% of these patients, though this finding may not be generalizable to patients in other hospitals. In patients with inflammatory arthritis, 63% were subsequently diagnosed with a RD, suggesting that ANA testing may be a useful clue in evaluation. Inpatient ANA testing should be reserved for cases with high clinical suspicion for an underlying RD rather than as screening for autoimmune conditions in inpatients.