Background: Understanding current practice patterns is essential to identifying opportunities for improvement and acknowledging good practice behaviors. However, often this information is not easily accessible or provided in a timely fashion, especially to front line staff. Key Performance Indicator (KPI) Boards are an effect tool to display timely data and are often used with nursing and support staff, but not for physicians.
Purpose: The aim of the project was to develop a method to reliably deliver quality data to front line providers in a timely and meaningful format through the use of KPI Boards.
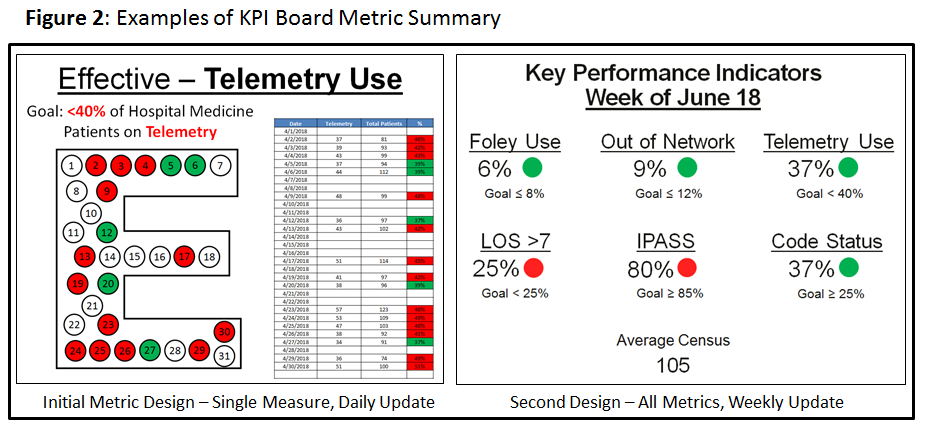
Description: The project was completed a large urban, academic medical center with a large direct-care and teaching hospitalist practice. Initial metrics for the KPI Board were selected based on data easily accessible in the electronic medical record on a daily basis. Foley catheter use, cardiac telemetry use, length of stay, out of network status, and updated handoff information were selected for initial inclusion. Metrics were linked to the Institute of Medicine STEEP framework, which was also used at the hospital-level. Initial goals for each metric were selected based on brief pilot data collection and the hospital medicine group’s goals. The metrics were displayed on unused wall-mounted monitors on a repeating slideshow within both major workrooms (Figure 1). KPI boards were put into use without specific instruction to determine level of passive acknowledgement. After a month of continued use, the metrics were reviewed by the group’s quality improvement committee to reset goals and adjust definitions of current metric and formal group education was provided. In addition to each metric, the boards were also used to provide reinforcement for ongoing quality improvement projects related to the metrics, such as reminders to review telemetry orders. The boards were utilized on a regular basis starting in February 2018. Based on provider feedback to appearance and technology limitations, the metric displays were transitioned from single metrics per slide daily to all metrics, single slide updated weekly (Figure 2). Data collection from multiple metrics was able to be used for ongoing quality improvement projects, telemetry reduction and quality handoffs, while it also supported stable compliance with hospital-level quality goals for Foley use. Qualitative feedback from providers was universally positive and generated significant discussion around the selected measures.
Conclusions: KPI boards are a novel means of displaying current quality data to hospital medicine providers. Weekly, rather than daily, updates were more feasible and better understood by providers. Metric data collection for KPI boards easily supports ongoing and future quality improvement projects.