
Background:
The incidence of in‐hospital cardiac arrest (IHCA) in the United States is unknown but has been estimated using administrative data from large nationally representative samples such the Medicare and Nationwide Inpatient Sample databases. However, the use of claims data has not been validated for this purpose. We aimed to measure the accuracy of inpatient claims data in determining IHCA incidence.
Methods:
A prospective observational study of adult IHCAs was conducted between January 2006 and July 2009 at a university teaching hospital. During that time, investigators tracked every activation of the cardiac arrest response team, excluding events in the operating or emergency rooms (where the team is not routinely activated). Administrative records were downloaded for every hospital admission over the same period and searched for ICD‐9 diagnostic code 427.5, procedural codes 99.60 and 99.63, and a pharmacy crash cart restocking fee. These were compared against our prospective gold standard for index arrests only.
Results:
There were 73,111 admissions and 704 index IHCAs, yielding an incidence rate of 9.6 IHCAs per 1000 admissions. The 2 procedure codes were not utilized during this period, but 466 admissions were billed for ICD‐9 427.50, of which 300 were confirmed prospectively (see Table 1). However, the restocking charge was utilized in 544 instances, of which 406 were true instances. Table 1 shows the sensitivity, specificity, positive predictive value, and negative predictive value for each of the measures, individually and combined. Using the ICD‐9 code alone would have yielded a calculated incidence of 6.3.
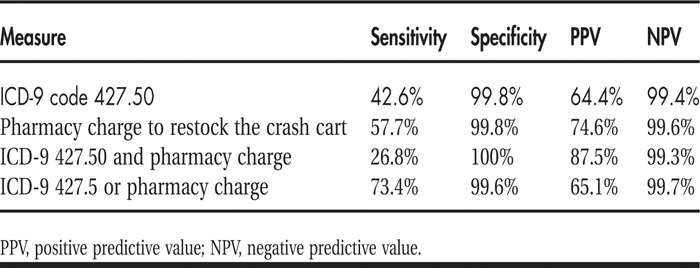
TABLE 1 Sensitivity and Specificity of Billing Data
Conclusions:
Standard administrative data likely underestimate the true incidence of IHCAs. Incidence rates based on these data should be interpreted with this understanding.
Disclosures:
D. P. Edelson ‐ National Heart Lung Blood Institute, research funding; Philips Healthcare, research funding; Program for Resuscitation Education and Patient Safety, honoraria; Sotera Wireless, consultant/advisory board; Sudden Cardiac Arrest Foundation, consultant/advisory board; T. C. Yuen ‐ none