
Case Presentation: 61-year-old female with history of asthma, hypothyroidism and migraines presented with 6 weeks of intractable headache, nausea and metallic taste. Provoking factors included standing upright and Valsalva maneuvers. Palliation occurred with lying flat. Anti-inflammatories, butalbital-acetaminophen-caffeine and triptans were ineffective outpatient. In the emergency department, IV fluids, ketorolac, diphenhydramine, metoclopramide, magnesium, ketamine and fentanyl were also ineffective. MRI of the brain with gadolinium showed diffuse pachymeningeal thickening/enhancement, cerebral sulcal/basilar cistern effacement, increased superior convexity of the pituitary gland, decreased mamillopontine distance, and slight cerebellar tonsillar ectopia compatible with intracranial hypotension. Investigation for spinal cerebrospinal fluid (CSF) leak was pursued with MRI of the entire spine. Several nerve root diverticula were seen; no active leak was identified. Consideration was given to invasive testing with CT myelography; the patient opted for empiric treatment with nontargeted blood patch which did bring some relief.
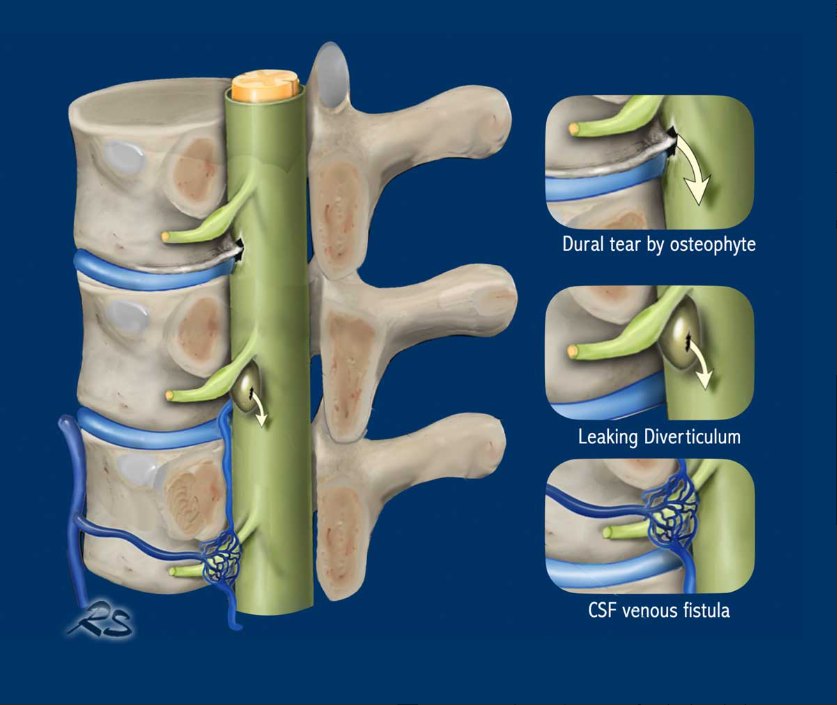
Discussion: Spontaneous intracranial hypotension (SIH) is a disabling condition caused by CSF leak. Incidence is 3.8 cases per 100,000 per year, with a 2:1 female predominance. The most frequent symptom is headache which worsens when upright and subsides when supine. It is frequently misdiagnosed as migraine. Headache is thought to result from efflux of CSF in the upright position, leading to traction on pain-sensitive fibers within the dura mater. Diplopia, dysgeusia, and vestibulocochlear disturbances are felt to be due to brain sagging and traction on the cranial nerves. Spontaneous CSF leak can be caused by calcified disc protrusion or osteophyte penetrating the thecal sac, leaks from spinal nerve root diverticula and direct CSF-venous fistulas. Neuroimaging is crucial in diagnosing SIH. Typical findings of intracranial hypotension seen on MRI brain include diffuse pachymeningeal enhancement, engorgement of venous sinuses, pituitary enlargement, and brain sagging (effaced suprasellar and prepontine cisterns and reduced mamillopontine distance) as seen in our patient.In contrast to iatrogenic CSF leak from lumbar puncture or surgical intervention, in SIH the site of leak is unknown. Evidence of intracranial hypotension on brain MRI should prompt search for the site of CSF leak.Whole-spine MRI can identify an extradural CSF collection, which indicates the presence of CSF leak but does not identify the site of leakage. Invasive testing with lumbar puncture and injection of iodinated contrast into the thecal space followed by ultrafast CT myelography is more effective at showing the contrast material escaping the dural sac in real time. Once the site and type of leak is identified, treatment consists of targeted epidural blood patch, surgical closure or transvenous embolization. If the site of leak cannot be identified, treatment is high-volume nontargeted epidural blood patch.
Conclusions: SIH is a debilitating disease that is often misdiagnosed as migraine, meningitis, psychological disorder, or even malingering. Targeted treatment is more effective than empiric treatment, and most effective if performed within 2 weeks of symptom onset. By considering SIH in all patients with orthostatic headache, the astute hospitalist can prevent delay in diagnosis and significantly impact morbidity in this patient population.
.png)