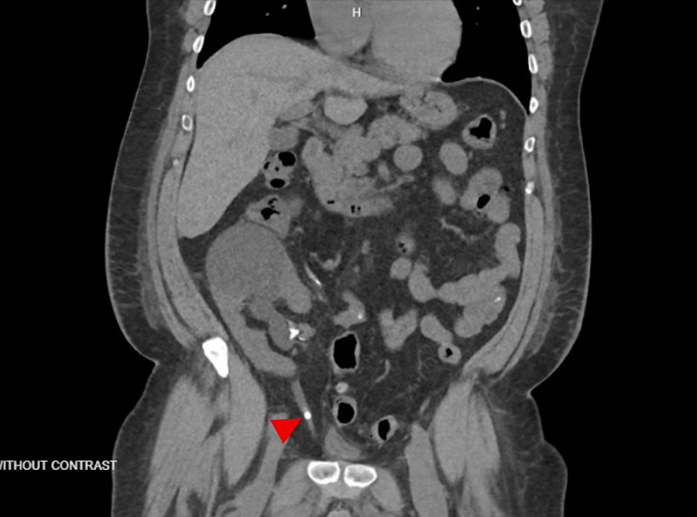
Case Presentation: A 48-year-old Native Hawaiian male with end-stage renal disease (ESRD) due to hypertensive nephrosclerosis, status post deceased-donor renal transplant (DDRT) complicated by a post-obstructive small bowel obstruction (2020), presented with a 3-day history of profuse non-bloody watery diarrhea. He reported poor oral intake, subjective fevers, and oliguria but denied nausea, vomiting, or abdominal or flank pain and had no clear triggers, including undercooked food, sick contacts, recent travel, medication changes, or NSAID use. On initial evaluation, his vitals were normal, and the physical exam was unremarkable without abdominal or CVA tenderness. Laboratory studies showed creatinine 32.0 mg/dL (baseline 3.6), BUN 165 mg/dL, potassium 6.1 mmol/L, bicarbonate 7 mmol/L, venous pH 7.19, and phosphate 13.4 mg/dL. Infectious stool studies, viral testing, hepatitis panel, CMV PCR, and BK virus PCR were negative. A renal ultrasound showed mild pelvic prominence but no hydronephrosis; however, CT imaging revealed a right-lower-quadrant transplanted kidney with a 6 mm obstructing ureteral calculus causing moderate hydronephrosis [Figure 1]. Interventional radiology placed a nephrostomy tube, resulting in post-obstructive diuresis and improvement in renal function. The patient’s diarrhea resolved with supportive care, and he was discharged for urologic follow-up for definitive stone management.
Discussion: Kidney stones are a rare but clinically significant complication after renal transplantation with an incidence of ~1.4-1.7% [1,2]. Risk factors include urinary infections, gout, prior nephrolithiasis, metabolic derangements, and graft-related anatomical challenges. Because transplanted kidneys are denervated, patients may not experience the classic renal colic symptoms, and stones may be discovered incidentally. However, oliguria, a rise in creatinine, and fever should prompt consideration of obstructive nephrolithiasis. Our case illustrates how coexisting gastrointestinal symptoms and an initial negative ultrasound can obscure the diagnosis of obstructive uropathy. Thus, CT imaging plays an important role if clinical suspicion persists. Management depends on the stone size, with stones < 5 mm managed conservatively, while ureteroscopy or percutaneous nephrolithotomy are reserved for larger stones. Overall, outcomes are favorable, with no significant reduction in graft survival when stones are appropriately treated [1-3].
Conclusions: In kidney transplant patients, unexplained acute kidney injury and oliguria should raise suspicion for obstructive nephrolithiasis, even without classic pain symptoms. When ultrasound is unrevealing, consider further imaging. Prompt recognition and treatment can lead to full recovery and prevent irreversible graft injury.