Background: Quality improvement and patient safety (QI/PS) is a major focus for hospitalists in both their day-to-day clinical care. In addition, many hospitalists have educational and administrative QI/PS duties, and salary support for them is highly sought after. As part of an ongoing effort to help identify opportunities to further support members of the Society of Hospital Medicine (SHM) QI Special Interest Group (SIG), known as QI Enthusiasts, a survey was conducted of its membership, which included information on salary-supported QI/PS roles. The aim of this study was to describe the population of QI Enthusiasts and to compare what features separated those with and without salary support for QI/PS work.
Methods: A survey was created by the SHM QI SIG Initiatives subgroup to elicit descriptive information of the SIG’s membership in relation to their current clinical, educational and administrative duties, and specifically how those roles intersect with QI/PS. The project received an exemption from the Montefiore Health System Institutional Review Board. The survey was created in a web-based platform that is licensed through SHM. Invitations to the survey were posted within the QI SIG forum on HMX, which is only seen by SIG members, and in the Open forum of HMX, which is seen by all HMX members. Notifications of the survey posting and subsequent messages on HMX are delivered to members who have opted into receiving email updates on various frequencies. The survey was not sent directly to any SHM members. After 6 weeks, including 2 rounds of reminder posts, the surveys were reviewed for the initial analysis. Comparisons of proportions of descriptive categories between those with and without salary support for QI/PS work was completed using Fisher’s Exact Test.
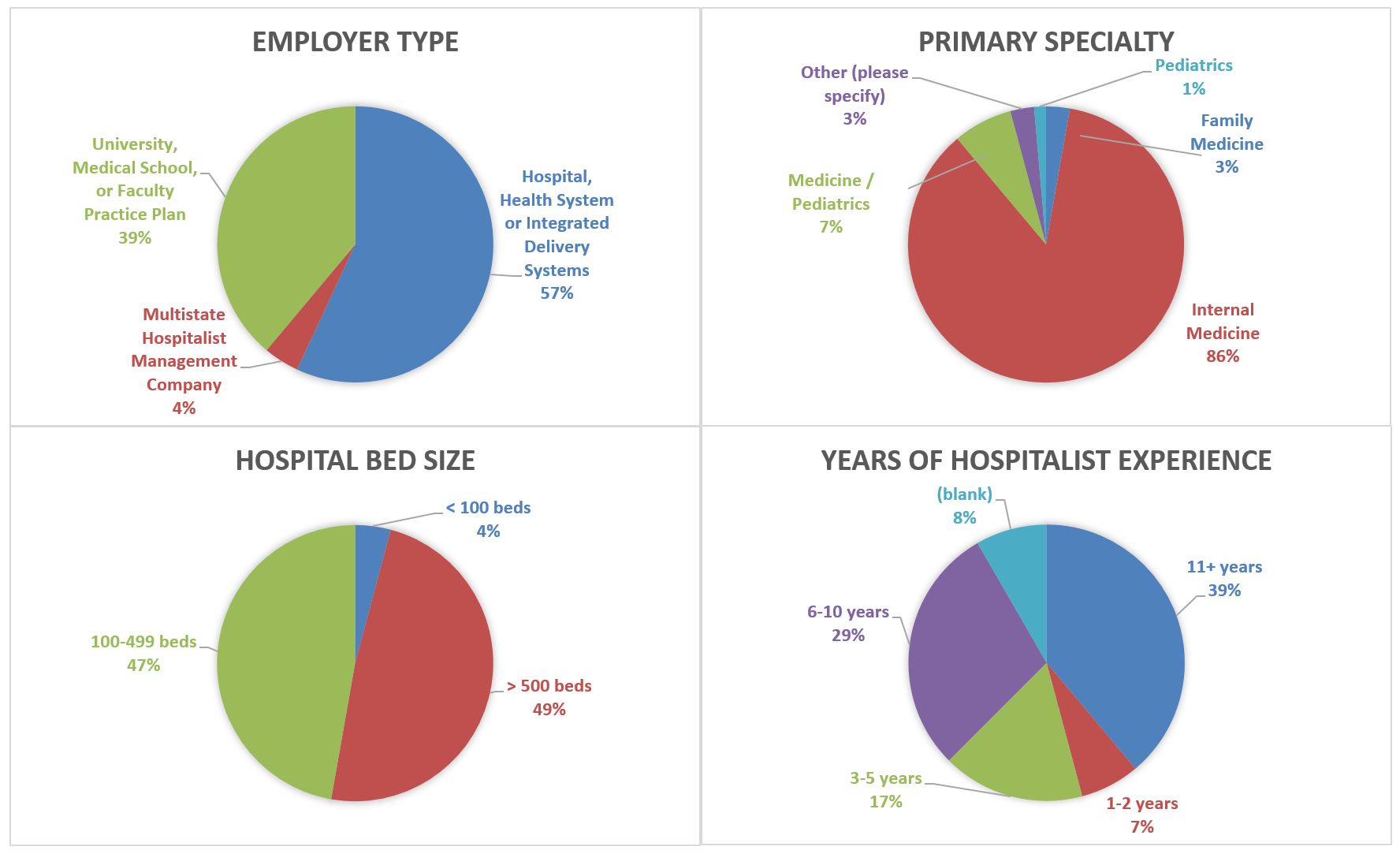
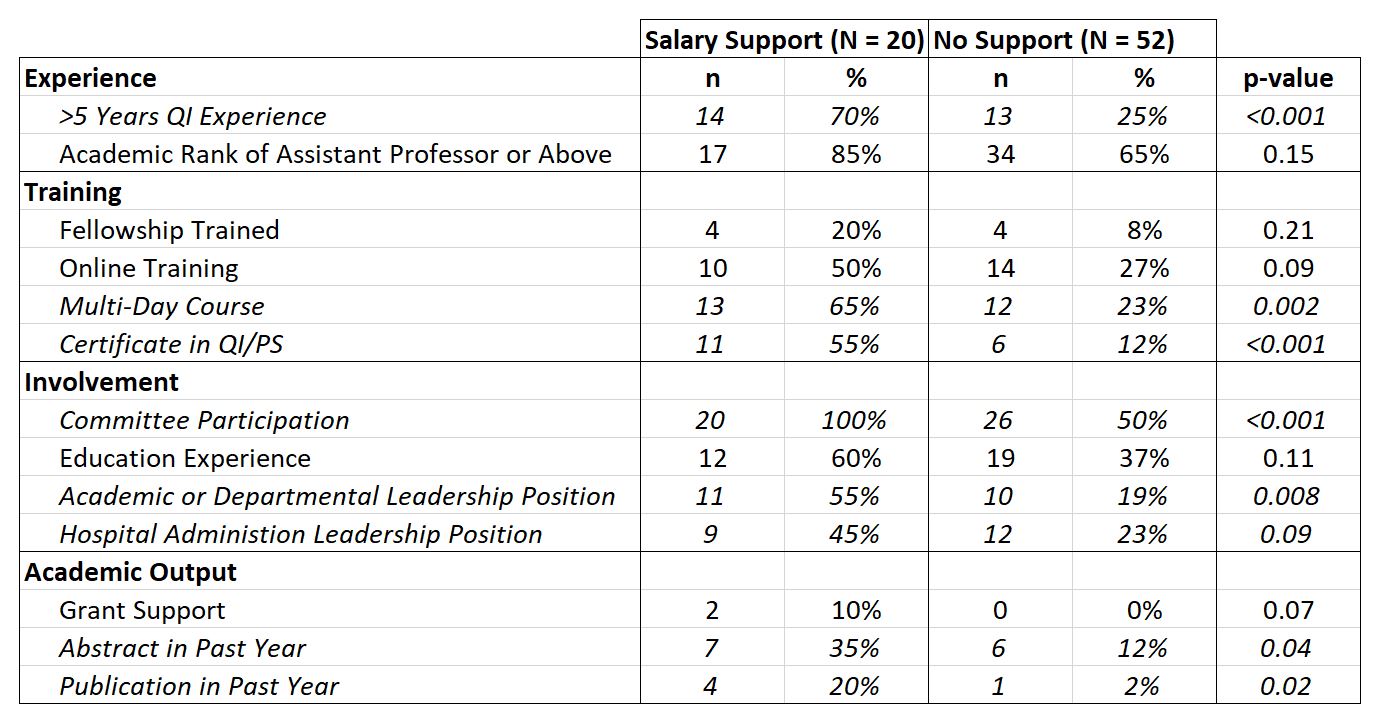
Results: A total of 72 SHM HMX members responded to the survey. Among the respondents, the most frequent employer was health systems (57%), nearly all were Internist (86%), and nearly 50% from >500 bed hospitals, but there was a wide range of years of clinical experience. Further details of the respondents’ practice environments, specialties, and years of QI experience are summarized in Figure 1. Twenty respondents (27.8%) stated they received salary support for QI/PS work at their institution. Hospitalists with salary support were significantly more likely to have over 5 years of QI/PS experience (70% vs 25%, p<0.001), but there was no significant difference in the proportion with or without an academic rank. All respondents with salary support had committee participation compared with only half of those without support (p<0.001). Those with abstracts or published articles were uncommon in both groups, but still significant higher in those with salary support (Figure 2).
Conclusions: HMX QI Enthusiasts are predominantly junior Internal Medicine faculty at large hospitals in healthcare systems or academic centers. Those who have salary support for QI/PS activities, in our sample population, are more likely to have intensive QI/PS training, hospital and/or academic leadership positions, and disseminated academic products in the past year. These specific differences may serve as points of focus for early career hospitalists who aim to have a salary supported QI/PS position.