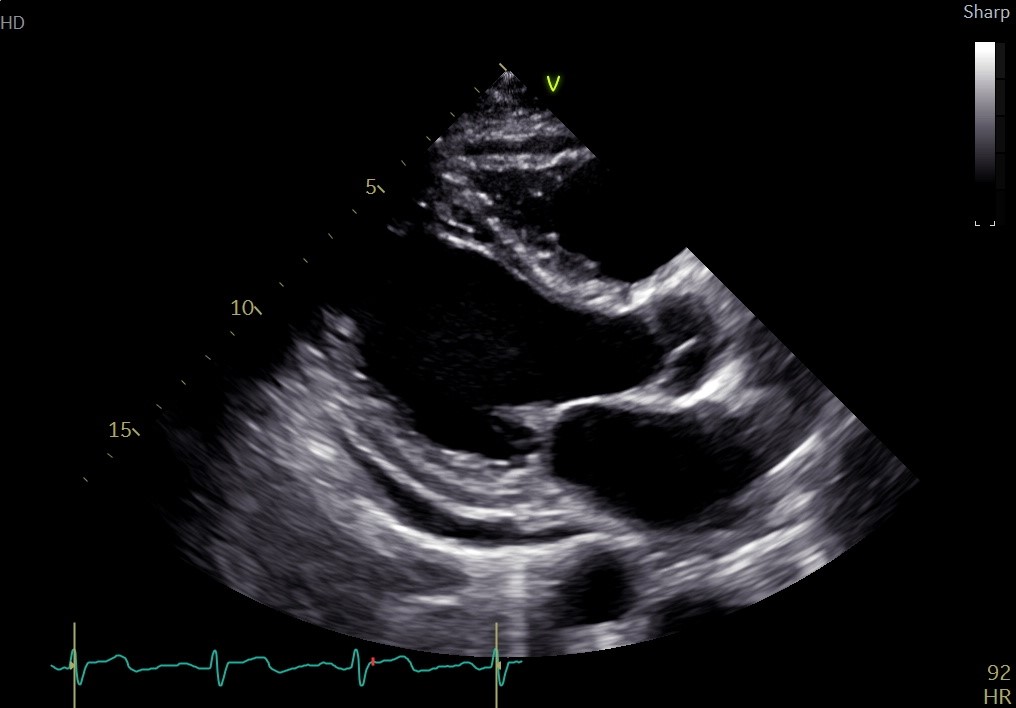
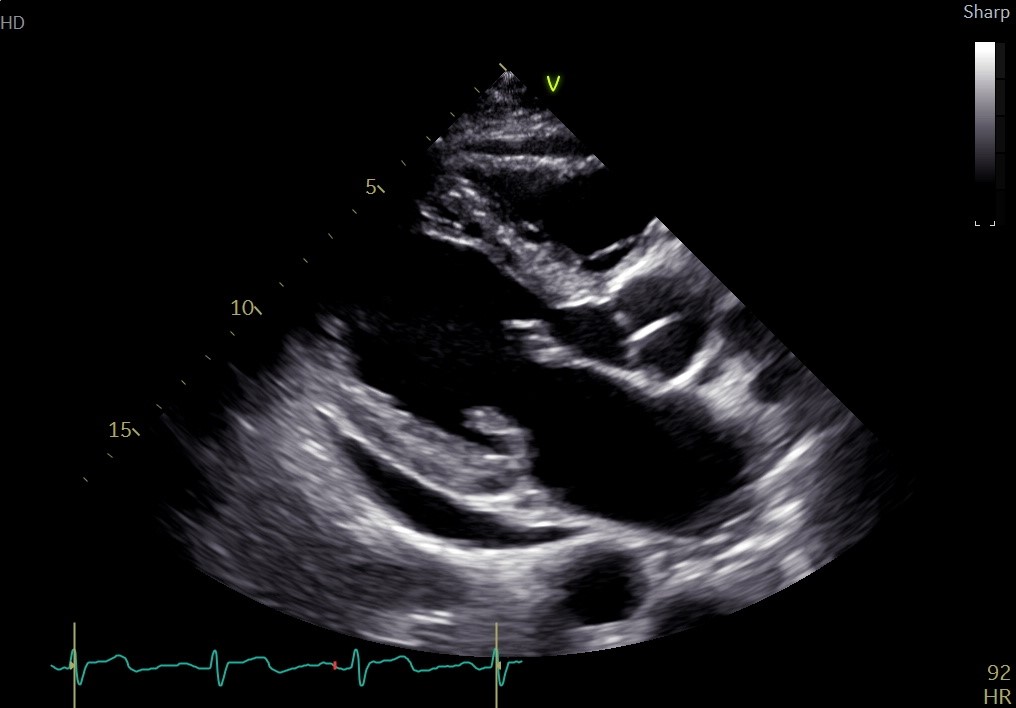
Case Presentation: A 50-year-old male with a history of hypertension, hyperlipidemia, and mitral valve prolapse presented to the ED per ophthalmology for further evaluation after 2 weeks of progressive bilateral vision changes, floaters, eye redness, and pain. On his initial presentation to eye clinic, he was diagnosed with bilateral panuveitis and managed with hourly prednisone eyedrops, daily atropine eyedrops, and intravitreal antibiotics. He also endorsed months of fatigue, night sweats, fevers, cough, weight loss, and a history of dental caries. On arrival to the ED, vital signs were normal and physical exam revealed right cervical chain lymphadenopathy, holosystolic murmur at the cardiac apex, and splenomegaly. Ocular exam revealed a fixed, irregularly shaped right pupil with no light perception, and a dilated left pupil with hypopyon that could only discern hand motions. Labs were notable for a CRP 148 mg/L and WBC 10.2k /uL with neutrophilic predominance. Outpatient blood cultures grew Aggregatibacter spp. after 49 hours and he was started on a 4-week course of 2 g IV ceftriaxone. A transthoracic echocardiogram found posterior mitral valve leaflet prolapse, a 1.2 x 0.8 cm mass on the anterior mitral valve, and moderate-to-severe mitral valve regurgitation. Due to vegetation size and regurgitation severity, he was a candidate for same-hospitalization mitral valve annuloplasty. In the interim, he was started on 60 mg prednisolone daily for ocular inflammation. His hospitalization was complicated by atrial fibrillation with rapid ventricular response, rate-controlled with metoprolol and diltiazem. His mitral regurgitation resolved with his valve repair. He received an outpatient vitrectomy and his vision has continued to improve.
Discussion: Aggregatibacter species are members of the HACEK group of gram-negative bacteria, which are part of the normal oropharyngeal flora.1-3 HACEK organisms are responsible for 1.5-2% of all cases of infective endocarditis and typically affect patients with underlying heart disease or prosthetic valves.1 Symptoms present insidiously and culture growth is slow. Aggregatibacter spp. are the second most common cause of HACEK endocarditis, often due to dental procedures or tooth decay.1,2,4 The mortality is low if caught early enough and treated with intravenous cephalosporins (4-6 weeks).5,6 Early surgical consultation to assess candidacy for same-hospitalization surgery is helpful in the setting of severe valve dysfunction, large vegetation, and clinical heart failure.6,7 Microvascular septic emboli have been a reported consequence of unaddressed infection.4,7,8 Endophthalmitis is intraocular inflammation due to infection that can be rapidly progressive and is associated with a poor visual prognosis if not treated early.9,10 Endogenous etiologies due to hematologic spread of infection account for only 2-8% of cases.10 Only a handful of reports exist of Aggregatibacter-induced endophthalmitis.10-13 In addition to treating the underlying bacteremia, intravitreal antibiotics and vitrectomy are used for treatment.10
Conclusions: HACEK spp. are a rare cause of endocarditis resulting in endogenous endophthalmitis. Hospitalists should have a high index of suspicion for subacute endocarditis when a patient presents with bilateral intraocular inflammation and vague systemic symptoms. Early diagnosis and surgical consultation of endocarditis during the hospital stay are key to ensuring good outcomes.