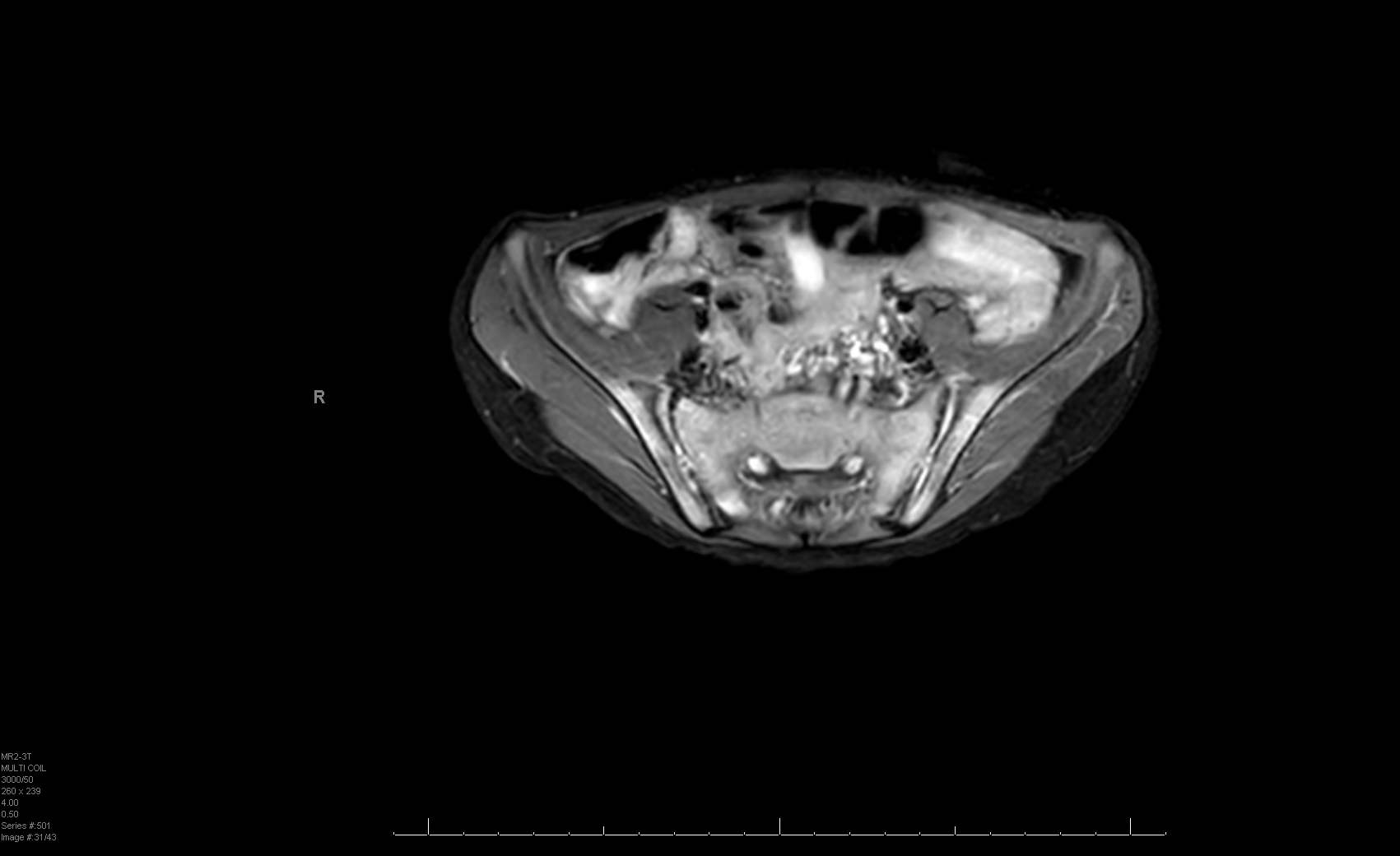
Case Presentation: 7-year-old male with asthma presented with an 8-month history of knee, hip, buttock, and back pain. Pain was worse in the morning and made it difficult for the patient to get out of bed. He was initially referred to physical therapy (PT) by his pediatrician. Pain worsened despite PT, and he was referred to neurology clinic for neuromuscular workup. Neurology workup included MRI of the brain and spine, EMG, and genetic testing, all of which came back normal. Over the month-long course of this workup, the joint pain worsened, and the patient became stiffer, prompting a referral to rheumatology. At the rheumatology visit, the patient’s mother reported new-onset watery diarrhea without blood, with up to 5 daily episodes and nighttime awakening, for the past month. The patient’s mother also endorsed 3lbs of weight loss (6% decrease) in the prior 5 weeks. Given this, the patient was directly admitted to the hospitalist service from rheumatology clinic. Upon admission, he was afebrile and thin appearing, with a soft, flat abdomen that was mildly tender to palpation. He had bilateral lower extremity weakness, worse in the right leg. Strength was most decreased with right hip flexion and leg extension. He had abnormal gait, with movements to circumvent right hip and knee use. The differential was broad, including inflammatory bowel disease (IBD), myositis, celiac disease, thyroid disease, and rheumatic disorders. Key lab work demonstrated normal WBC, elevated CRP, ESR, and LDH. Stool ova/parasite and culture were negative, and fecal calprotectin was elevated to 1690ug/g. MRI of the lower extremities and pelvis demonstrated bilateral sacroiliitis (Fig. 1), left knee effusion with enhancing synovitis, edema of the left femoral head, and small pelvic fluid. Endoscopy and colonoscopy were performed and visually normal. Pathology demonstrated inflammation throughout the GI tract with eosinophilic esophagitis, gastritis, duodenitis, terminal ileitis, mild colitis from cecum to sigmoid colon, and moderate inflammation in the rectum. A new diagnosis of Crohn’s Disease was made and the patient started on infliximab.
Discussion: IBD has a rising prevalence in in the United States, frequently presenting with extraintestinal manifestations (EIMs) (1, 2). Musculoskeletal involvement is the most common EIM of IBD, affecting up to 30% of individuals, with a similar trend observed in the pediatric population (3, 4). Presentation of axial joint involvement can vary from asymptomatic, incidental findings to more severe sacroiliitis. Sacroiliitis (SI), an inflammatory arthropathy of the sacroiliac joints, can present with nonspecific symptoms such as low back pain, stiffness, or buttock pain, as observed in this patient. Children with Crohn’s disease (CD) appear to be more prone to sacroiliitis compared to those with ulcerative colitis (4). Notably, sacroiliac involvement in pediatric CD often manifests without direct correlation to disease activity, as seen in this case (5). To our knowledge, this is the first reported pediatric case in which axial joint involvement preceded gastrointestinal symptoms, underscoring the need for comprehensive assessment in pediatric patients presenting with musculoskeletal pain.
Conclusions: Pediatricians should maintain a broad differential when managing patients with arthritis or other extraintestinal manifestations of IBD, even in the absence of GI symptoms.