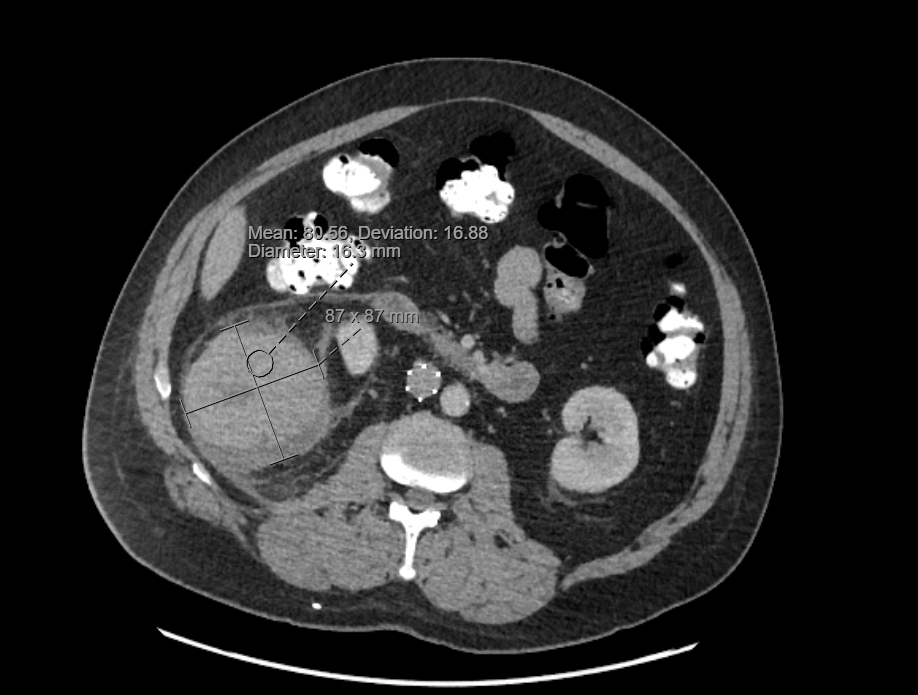
Case Presentation: A 60-year-old man presented with four days of right upper quadrant pain and right flank pain. He had a past medical history that included hypertrophic cardiomyopathy with pacemaker and ICD, hyperlipidemia, atrial flutter, hypertension, prior pulmonary embolism status post IVC filter, and a known renal cyst first identified greater than ten years prior. He had recently returned from a trip to Costa Rica, where he experienced a sudden, severe onset of RUQ abdominal pain with radiation to his right flank. The pain was constant but worse with movement and inspiration and was initially attributed to food poisoning by the patient. He denied any trauma to the region, particularly given that he had chronic difficulty ambulating due to multiple previous femur surgeries; he ambulated with crutches at baseline. He presented to care due to persistent and progressive pain. Vital signs on presentation were BP 131/81, HR 74, Temp 37.1°C, RR16. Physical exam was notable for RUQ tenderness to deep palpation and notable absence of costovertebral angle tenderness or skin discoloration/ecchymosis. Laboratory findings were notable for leukocytosis of 14.4 x1,000/uL and an initial hemoglobin of 10.1 g/dL from baseline of 12 g/dL. CT imaging showed a heterogeneously hyper-dense lesion in the lower pole of the right kidney measuring up to 9.9cm in size with surrounding stranding and fluid in the right perinephric space, likely reflecting the sequelae of a ruptured hemorrhagic renal cyst though solid component could not be excluded. Confirmation with MRI was delayed due to concerns regarding the patient’s pacemaker and retained spinal stimulator leads. He was normotensive and his hemoglobin remained stable through admission, and he was discharged with plans for outpatient MRI and nephrology evaluation.
Discussion: Here we present a case of a spontaneous, atraumatic hemorrhagic rupture of a renal cyst, also known as Wunderlich Syndrome. This is a rare clinical syndrome of acute onset of renal hemorrhage into the perirenal, pararenal or subcapsular spaces without history of antecedent trauma. In this case, the patient was aware of a known right renal cyst that was 2cm in size, last imaged 10 years ago, and denied any preceding trauma. In the hospital setting, it is rare to see cases of ruptured hemorrhagic cysts, and even rarer for patients to present with spontaneously ruptured renal cysts. Underlying causes of Wunderlich Syndrome include renal neoplasms, renal vascular aneurysms or AV malformations, renal vein thrombosis, and rarer still, renal infections, cystic disorders, or renal calculi. Management of Wunderlich Syndrome should focus on close evaluation of blood counts and vital signs to monitor for any developing hemorrhagic shock. MRI should be obtained to rule out malignancy as renal neoplasms such as clear cell renal cell carcinomas account for 60-65% of all cases of Wunderlich Syndrome.
Conclusions: In conclusion, it is important for the hospitalist to keep a broad differential during evaluation of patients with sudden-onset flank pain or upper quadrant pain, particularly with a known history of renal cysts. Any spontaneous ruptured hemorrhagic cyst identified on imaging should prompt concern for potential neoplasm of the kidney as they account for the majority of cases of Wunderlich Syndrome. Although Wunderlich Syndrome is rare, it can be life threatening if it progresses to hemorrhagic shock. Patients who meet this diagnosis should be monitored closely through frequent vital sign checks and laboratory monitoring.