
Case Presentation:
A 92‐year‐old woman with a medical history of recurrent urinary tract infections (UTIs) presented with progressive dyspnea, a dry cough, and low‐grade fevers for 6 weeks. She was taking nitrofurantoin for prophylaxis of recurrent UTIs for 3 months prior to the presentation. Relevant clinical findings included a respiratory rate of 28/minute, oxygen saturation of 88% on room air, and bilateral inspiratory rales in the lungs. A chest X‐ray and a CT scan showed extensive diffuse bilateral interstitial lung disease. Bronchoalveolar lavage (BAL) and a transbronchial lung biopsy were negative for infectious and neoplastic etiologies. An echocardiogram showed normal ventricular and valvular functions. A diagnosis of nitrofurantoin‐induced lung toxicity was made, and nitrofurantoin was stopped. Unfortunately, the patient died after 2 weeks from progressive respiratory failure.
Discussion:
Most patients affected with nitrofurantoin pulmonary toxicity are women. Elderly women are particularly at high risk. Clinical manifestations of nitrofurantoin pulmonary toxicity can be acute, subacute, and chronic. Acute presentation is common and is characterized by constitutional symptoms including fever, rash, arthralgia, and fatigue. Common pulmonary symptoms are dry cough, chest pain, and dyspnea. Acute reactions occur within 1 month on nitrofurantoin therapy. Subacute presentations as in this case have a more insidious onset of symptoms, with most reported cases having received nitrofurantoin for periods ranging from 1 to 6 months. Common symptoms include dry cough, dyspnea, low‐grade fever, and cyanosis. Chronic presentation and pulmonary fibrosis are seen in patients on nitrofurantoin therapy for more than 6 months, and the usual presenting symptoms are progressive dyspnea and dry cough over weeks to years. Fulminant pulmonary hemorrhage presenting with hemoptysis and respiratory failure has also been described. Although BAL is helpful to exclude infectious etiologies, BAL findings are nonspecific. Discontinuation of nitrofurantoin therapy generally results in the regression of symptoms; however, weeks to months may be required for recovery. Glucocorticoids are sometimes given as a therapeutic measure, although they do not seem to accelerate recovery.
Conclusions:
Nitrofurantoin pulmonary toxicity can present as an acute, subacute, or chronic respiratory disease. Common manifestations are dry cough, chest pain, dyspnea, and hypoxemia. Elderly women are particularly susceptible. Chest imaging shows patchy infiltrates and fibrosis. Treatment includes stopping the medication and occasionally a course of corticosteroid therapy. The prognosis is good if the condition is recognized early, and nitrofurantoin exposure is stopped; however, rare fatalities have been reported.
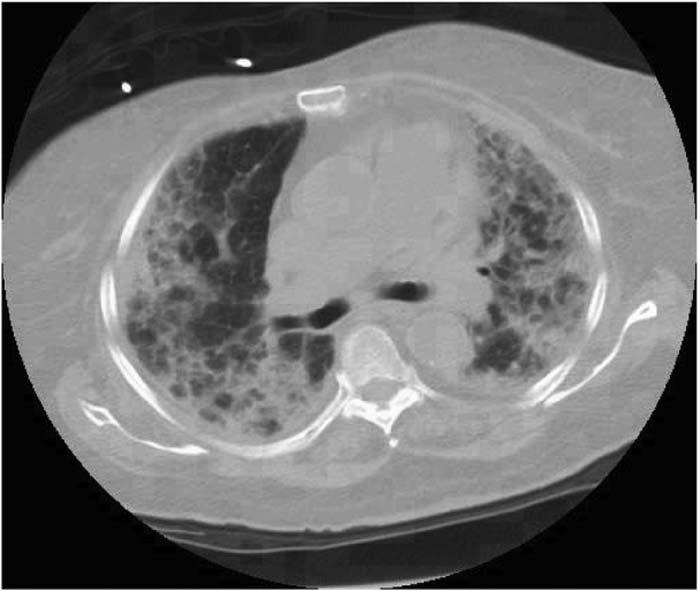
Bilateral ground glass attenuation is the classic CT finding of nitrofurantoin pulmonary toxicity
Author Disclosure:
C. Chaulagain, Prevea Clinic, Hospitalist.