Case Presentation:
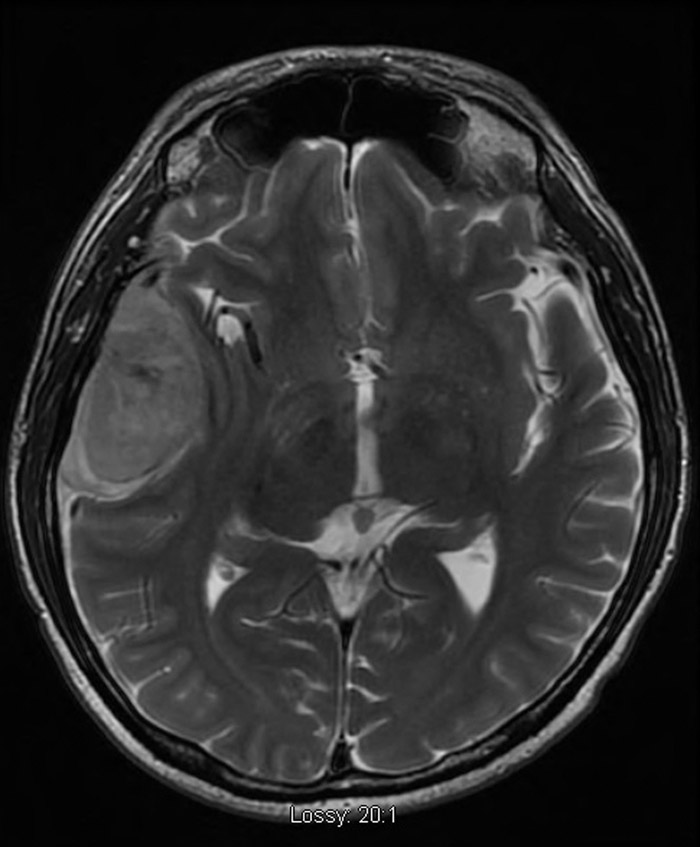
A 37‐year‐old male with AIDS (CD4 104) presented with progressive fatigue, associated with diarrhea, nausea, palpitations, and episodes of intermittent slurred speech for two months. Physical exam was unremarkable with the exception of 4/5 strength in all four extremities. Laboratory data revealed anemia (hgb 10g/dL) thrombocytopenia (44K/uL), hypercalcemia (12.4mg/dL), elevated lactate dehydrogenase (LDH 1219 U/L) and acute kidney injury (Cr 2.82mg/dL). CT of the head revealed a large right temporal mass with an adjacent subarachnoid hemorrhage and a right to left midline shift of 4mm. An MRI subsequently better defined this as a 3x6x4 cm mass suggestive of meningioma. CT scan of the chest and abdomen revealed a 4×5 cm left paramediastinal mass and multiple abdominal and pelvis masses with the largest measuring 4×4 cm. The findings of a midline shift coupled with the neurological symptoms led to an emergent craniotomy the next day.
A bone marrow evaluation revealed a lymphoproliferative (CD45+) process showing plasmacytic differentiation (CD138+, MUM+) that was negative for B‐cell markers and TdT. The brain mass showed a similar immunophenotype, and additionally lacked follicle center markers, CD10 and BCL6. Other significant negative markers were CD30, ALK1, MPO and HHV8. EBER was positive in the bone marrow specimen and negative in the brain mass. However, the process was deemed similar, and a diagnosis of plasmablastic lymphoma (PBL) was made.
Patient is currently undergoing treatment with high dose cytarabine and methotrexate alternating with EPOCH (Etoposide, Doxorubicin, Vincristine, Cyclophosphamide, and Prednisone).
Discussion:
PBL was first described by Decluse in 1997 and since then the WHO has identified it as a distinct subtype of large B‐cell Non‐Hodgkin Lymphoma mostly found in AIDS patients. Clinically patients with PBL tend to be young HIV‐positive men, who present with advanced disease, high LDH and extranodal involvement.
It is estimated that PBL accounts for approximately 3% of cases of HIV‐related non‐Hodgkin’s lymphoma. This disease normally presents in the oral cavity, however, extra‐oral sites have been documented including the lung, breast, skin and gastrointestinal tract. After an extensive Pubmed search, we found only one case report of PBL presenting as a basal ganglion mass.
Conclusions:
Over 150 case reports have documented occurrence of PBL however only 1 previous case report confirmed PBL as a central nervous system mass. This case features an unusual presentation of PBL and highlights the importance of considering this diagnosis in individuals with AIDS that present with a brain mass