Unnecessary Transfusions: Hospital Medicine Leading Institution Wide Change
Lesley Schmaltz MD, Shalini Bhattacharya MD, Jisu Kim MD, Amir Jaffer MD MBA, Amanda Tosto RN MS, Scott Hasler MD, Manya Gupta MD
Background:
It is well known that excessive blood transfusions can cause harm without improving clinical outcomes. As such, an evidence based restrictive transfusion guideline is recommended. A pilot study performed on the general medical floors at our institution showed that a hospitalist led intervention improved adherence to this latest standard of care and significantly reduced the number of unnecessary blood units transfused. Given the success of this project on our general medical floors, our hospitalist team broadened the initiative to incorporate the whole institution.
Purpose:
Our goal was to increase institution-wide adherence to a restrictive transfusion strategy for adult inpatients in all medical departments of our institution. The objectives included decreasing the percentage of patients transfused while admitted, the units transfused for hemoglobin (Hgb) >8g/dL, and multiple unit transfusions. Blood units transfused in operating rooms were excluded. Secondary goals were to reduce the cost associated with blood utilization and to demonstrate a substantial change in practice through a hospitalist led initiative.
Description:
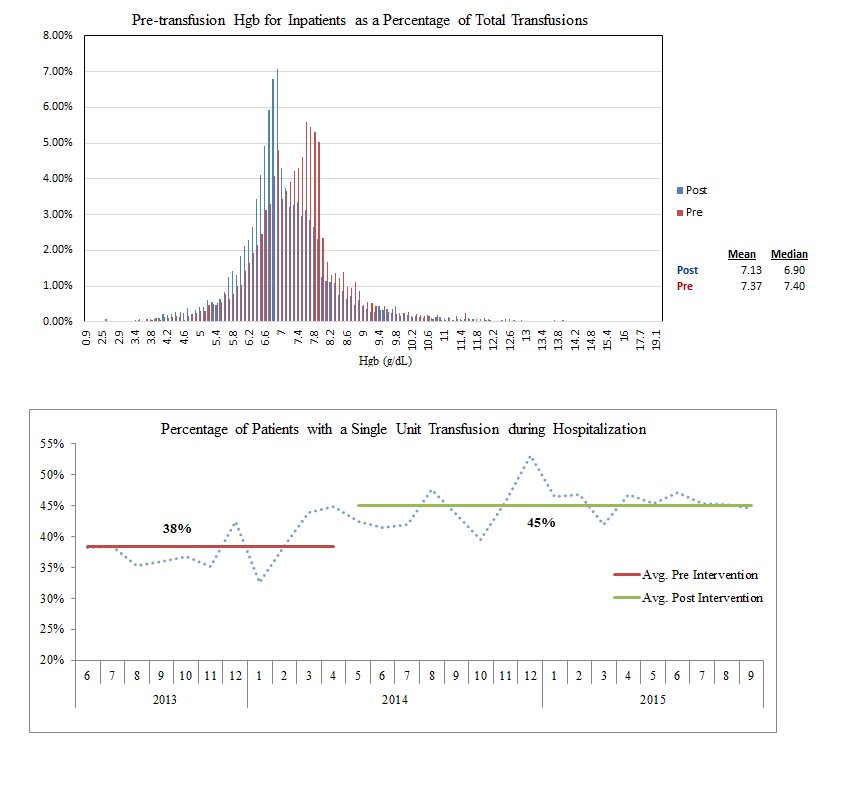
We promoted adherence to a restrictive blood transfusion policy by implementing modifications to the transfusion order set in our EMR, coupled with education on the specific indications for blood transfusions. Electronic communications were sent to all ordering providers at our institution as well as multiple educational sessions that focused on transfusion indications and safety. The initiative was launched in May 2014, and while data collection is ongoing, here we present 17 months of post-intervention data. We examined multiple metrics including Hgb levels at time of transfusion, percentage of inpatients with a single unit transfusion, and the cost-savings associated with adherence to a restrictive transfusion strategy.
Conclusions:
Our intervention demonstrated a significant and sustained reduction in blood utilization at our hospital. The mean Hgb at the time of transfusion decreased from 7.37 g/dL (pre-intervention) to 7.13 g/dL (post-intervention) with adjustments made for census. The percentage of patients with only a single unit transfused during hospitalization increased from 38% to 45% and the total percentage of patients receiving a transfusion during hospitalization decreased from 19% to 16% after our intervention. We noted an associated cost savings of over $400,000 during a 10 month post-intervention period. These findings indicate that hospitalists can be leaders in envisioning and creating a substantial and sustainable institution-wide change in medical practice through optimization of the EMR, education, and collaboration with other specialties.