Background:
Medical overuse, defined as the provision of services for which harms outweigh benefits, is increasingly recognized as a driver of high cost and poor clinical outcomes in the U.S. health care system. Despite increasing attention to overuse, methods for reducing it are unclear. In contrast, methods of identification, analysis, and prevention of medical errors have improved considerably since the pivotal 1999 Institute of Medicine report, “To Err is Human,” However, overuse has not been explicitly framed as a medical error so formal methods of analyzing errors have not been applied to the problem of overuse. A framework in which overuse is considered a medical error would facilitate understanding of the drivers of overuse and systems factors that lead to it.
Purpose:
Our purpose was to create a case conference to identify and analyze cases of overuse as a medical error, and to create a process for implementing systems change to prevent future overuse and harm.
Description:
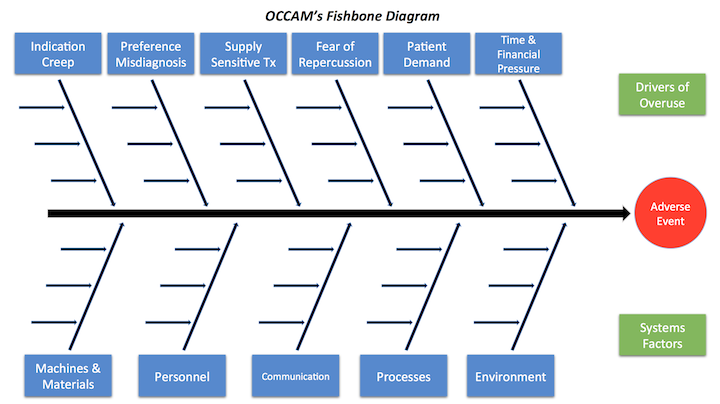
A monthly inpatient series called Overuse Clinical CAse Morbidity & Mortality (OCCAM’s) Conference was created. It is named after Occam’s razor, a principle of parsimony, economy, and succinctness used in problem solving. The audience is comprised of students, residents, faculty, and administrators. The case conference is based on inpatient medicine cases where overuse led to patient harm or near miss. Discussion on value and cost is moderated, with an emphasis on the patient’s social and financial history. A root cause analysis (RCA) is completed, utilizing a modified fishbone diagram (Figure 1) to explore 1) drivers of overuse and 2) systems factors. Finally, a brainstorm session is held to suggest methods of improving the system. The results of these conferences are conveyed to the OCCAM’s Workgroup, where hospitalists and trainees work together to implement actual systems change.
We evaluated attitudes toward overuse and cost-containment through surveys, which were collected from residents (n=95) prior to their first conference. Results include: “Trying to contain costs is the responsibility every physician” (93% agree); “Ordering unnecessary tests is NOT harmful to patients“ (95% disagree); “Faculty ask me to order tests I think are unnecessary” (5% disagree). Follow-up surveys will address attitudinal changes associated with conference attendance. Nine conferences were held. Topics of overuse included proton pump inhibitor use in steroids and ultrasounds for acute renal failure.
Conclusions:
OCCAM’s Conference provides a unique process to identify, discuss, and analyze cases of overuse as medical errors through a modified RCA format. It also provides a natural avenue for implementing systems change to decrease overuse and resultant excess cost and patient harm.