Case Presentation:
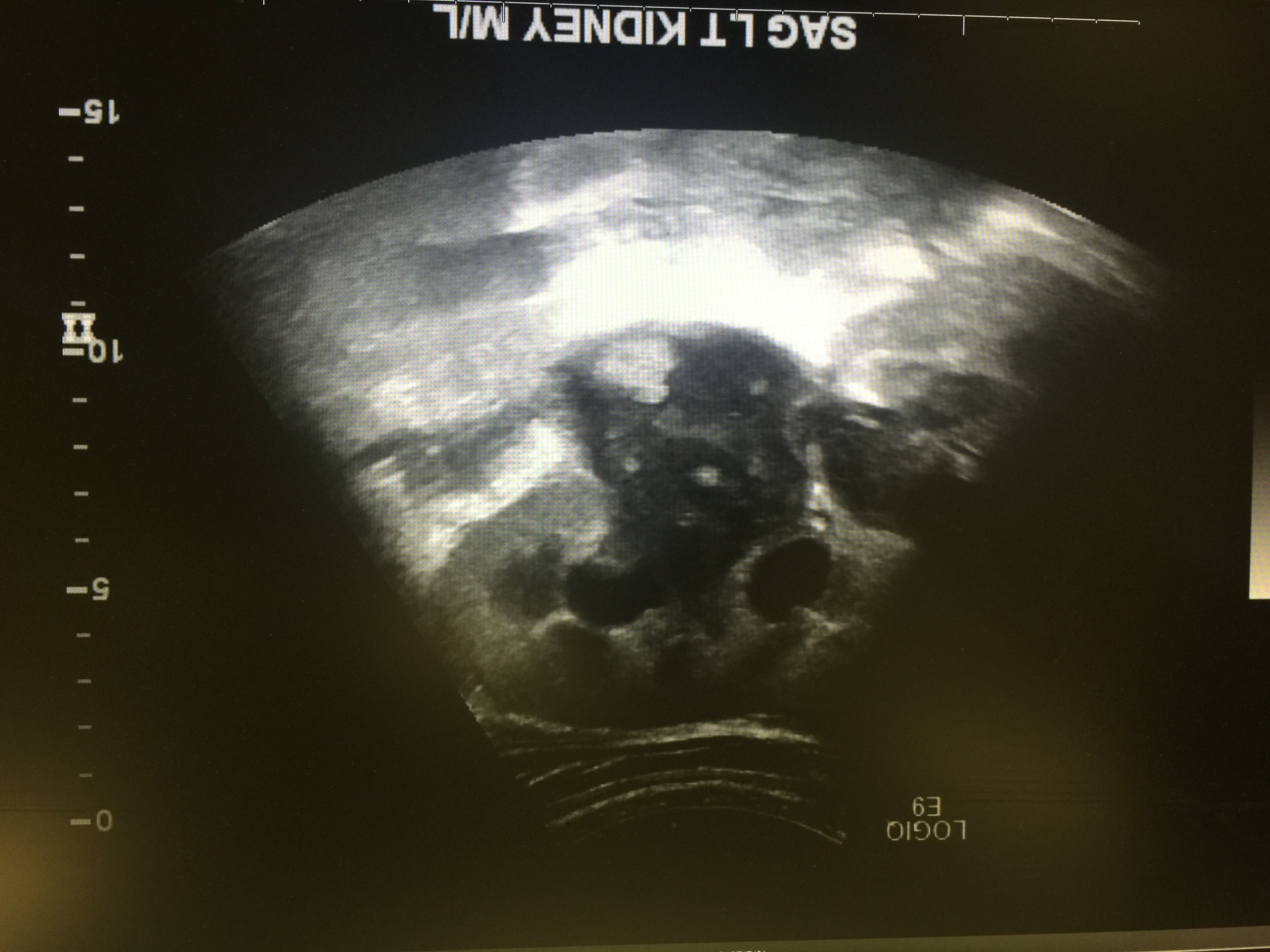
A 24 yr old male with PMH significant for uncontrolled DM and Hepatitis C presented with left sided flank pain and dark urine for 2 weeks. Lab workup was significant for leukocytosis and a negative UA. CT Abdomen showed left sided hydronephrosis, retroperitoneal adenopathy. Retroperitoneal adenopathy was believed to be the cause of hydronephrosis. A left JJ ureteral stent was placed by Urology team. Urine culture grew yeast, likely contaminant. Patient was discharged home pending workup for possible lymphoproliferative disease after Oncology consultation.Three weeks later patient presented with worsening left flank pain, workup showed leukocytosis,UA positive for LE and worsening left hydronephrosis on USG. Previous Workup for lymphoproliferative disease and viral and protozoal serologies was negative. Patient was started on Cefepime. Urology believed worsening hydronephrosis was due to detrusor hypo activity. After stabilization, patient was discharged home with foley catheter and PO antibiotics . Urine culture was negative for bacterial organism but positive for 50K yeast. Patient was not treated for possible fungal infection as again it was thought to be colonization. USG was repeated one week later which showed stable hydronephrosis but presence of round echogenic material in renal pelvis, highly suggestive of fungus ball. Patient was started on IV Fluconazole and IR guided nephrostomy tube was placed. During the procedure frank greenish fluid was noted in renal pelvis and Left JJ stent was noted to be occluded. Cultures from fluid grew Candida Albicans. Patient was discharged on Po Fluconazole and urological intervention was planned after 2 weeks of anti fungal treatment.Two weeks later, patient underwent percutaneous resection of fungus ball, removal of JJ stent and replacement of nephrostomy tube. A week later left side anterograde Nephrsotogram showed no obstruction, nephrostomy tube was removed. Patient continued Fluconazole for additional 1 week and did well after that.
Discussion:
Candiduria is frequently observed in patients with Diabetes, indwelling urinary catheters, prolonged antibiotics and immunosuppressive therapy. Neither the presence of pseudohyphae in the urine nor the number of colonies growing in the culture help to distinguish colonization from infection. Persistent candiduria especially in diabetics should prompt radiological imaging of kidney to evaluate for involvement.
A fungus ball originates from agglutination of necrotic tissue (papillary necrosis), mucus debris and foreign or lithiastic debris which can lead to obstruction at UP junction obstruction and hydronephrosis.
Obstructive urosepsis due to fungus mass requires appropriate drainage in the form of nephrostomy tube, which provides better access for collection of material for microscopic study, access to percutaneously remove fungal ball and administration of local antifungal agents.
Conclusions:
This case highlights the importance of candiduria in patient with uncontrolled diabetes. Although treatment of asymptomatic Candiduria is not indicated but the presence of abnormal urological and radiological findings in immunocompromised patients requires prompt investigation and treatment. Fungus ball of kidney is rare but potential complication of Candida UTI and requires medical, surgical therapy and aggressive control of underlying precipitating condition.