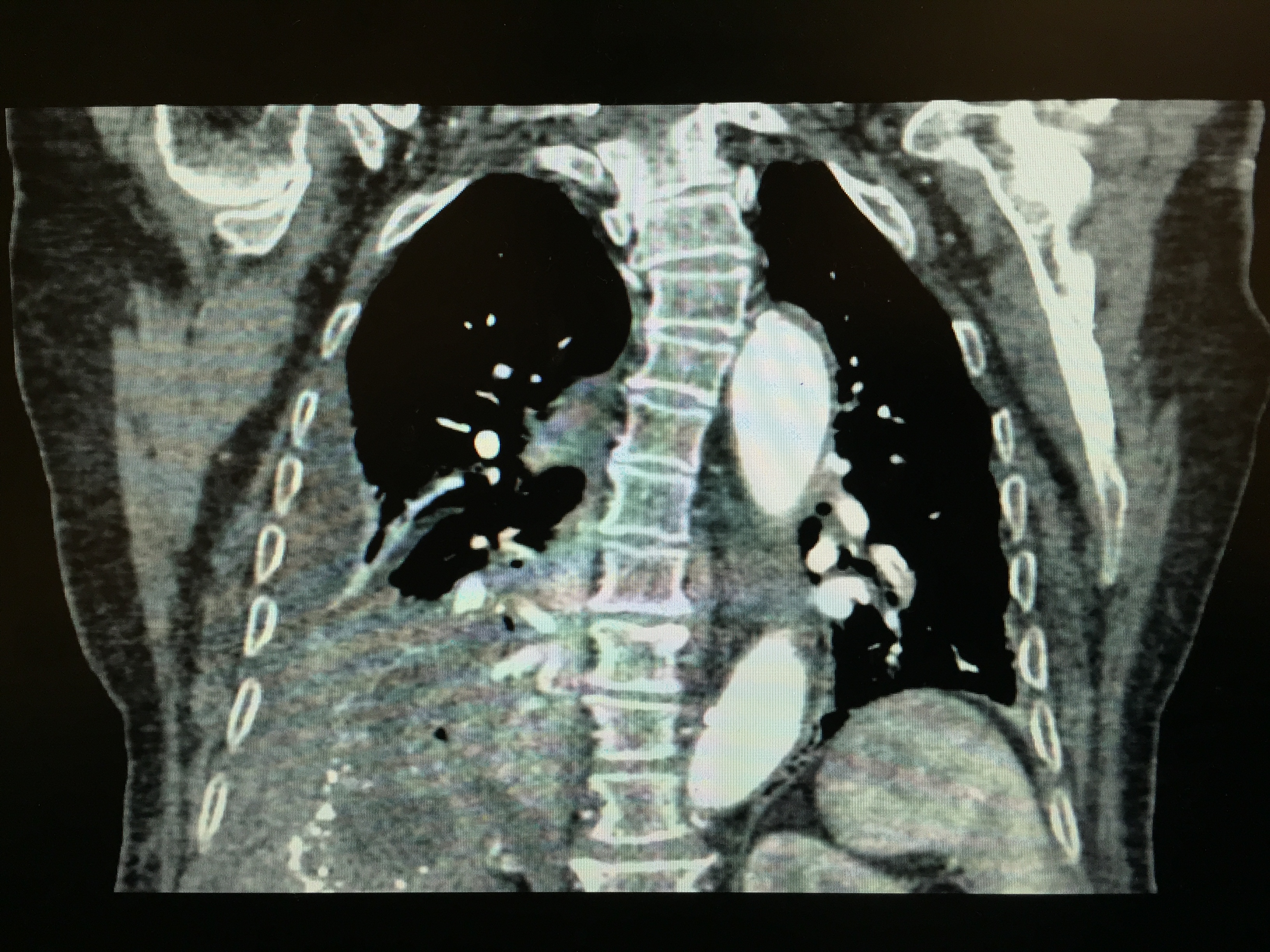
Case Presentation: An 85-year-old Middle Eastern woman with an intermittently treated solitary hepatic hydatid cyst diagnosed 40 years ago presented to a hospital for 1 month of progressive nausea, vomiting, abdominal pain, and new onset hemoptysis. Past history included multiple myocardial infarctions and an ischemic stroke. She immigrated to the United States (US) from a village in Iraq 18 months prior to admission. She was afebrile, hypotensive, and tachypneic with oxygen saturation of 94% on 3L oxygen via nasal cannula. She was in mild respiratory distress with decreased right lung base breath sounds associated with dullness to percussion. Remainder of her exam was unremarkable. Laboratory studies noted 9.0 WBC/mm3 (2% eosinophils), positive echinococcus (EC) antibody titers, and E. coli in sputum, for which a 4 week course of albendazole and ceftriaxone was initiated. CT imaging revealed a complex 8.7cm rim-calcified cyst in the superior right hepatic lobe communicating through a diaphragmatic defect into the right lower lung lobe with associated consolidation and loculated empyema. Bronchoscopy confirmed a hepatobronchial fistula (HBF) without biliary involvement. A poor surgical candidate, she underwent a puncture-aspiration-injection-reaspiration (PAIR) of the cyst with 3% saline and percutaneous cyst drain placement to water seal. Bronchial and cyst aspirates grew E. coli, and cyst fluid contained EC hooks and scolex. Her course was complicated by post-PAIR septic shock and respiratory failure from hypoventilation. A post-PAIR day 12 CT noted improved right lung consolidation with possible HBF tract closure. The patient’s family opted against further intervention due to risks of a fistula closure procedure and prolonged intubation. She was successfully extubated.
Discussion: EC infection is an emerging health problem in the US amongst immigrant populations from endemic regions such as the Middle East. Chiefly affecting the liver (67%) and lungs (25%), EC typically remains asymptomatic, but patients may develop complications including biliary obstruction, secondary bacterial infections, anaphylaxis from cyst rupture, and rarely, fistula formation. This case describes a potentially deadly complication of hepatic EC, seen in 2% of cases in European studies. HBFs seldom occur due to dense adhesions between the parietal pleural and cyst. Biliary irritation and favorable pressure gradient toward the intrathoracic space are suspected to facilitate diaphragmatic rupture. First-line therapy includes surgical fistula closure with diaphragmatic repair. However, PAIR with percutaneous catheter drainage may be an effective alternative in inoperable patients.
Conclusions: This case highlights the importance of recognizing EC as an emerging concern in the US, its complications, and the multidisciplinary management. With a growing influx of immigrant populations from endemic regions, providers must consider EC and its complications in at-risk patients.