Case Presentation:
A 54-year-old female with hypertension and tobacco use presented with two months of new onset constipation and progressively worsening, diffuse, generalized abdominal pain, early satiety, and a 30-pound weight loss. She was found to be anemic. A colonoscopy was performed that was unremarkable. Two months later, with no symptomatic improvement with laxatives, she developed flank pain, decreased urinary output and was admitted to an outside hospital with acute kidney injury and imaging consistent with bilateral hydronephrosis.
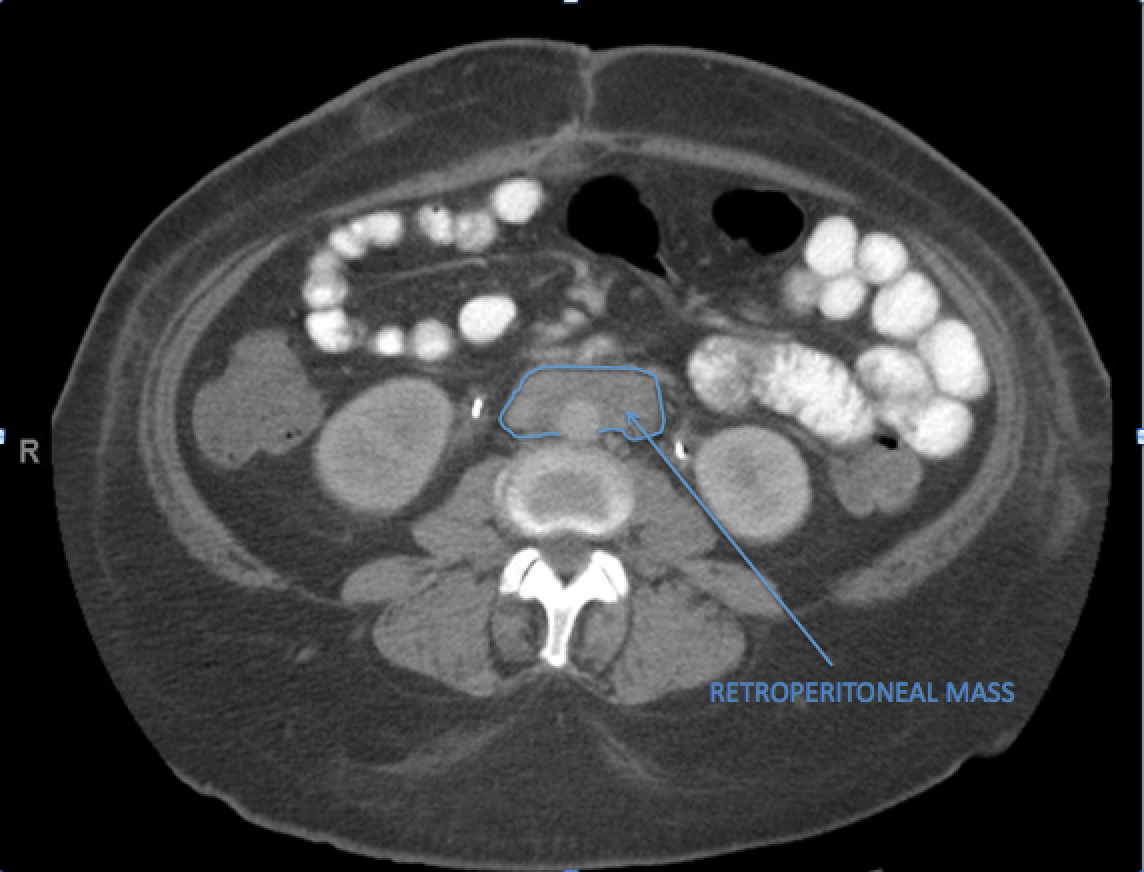
On CT, retroperitoneal lymphadenopathy versus a mass was seen. Bilateral ureteral stents were placed. A PET scan showed a “mantle of conglomerated neoplasm” in the retroperitoneum. Due to concern for lymphoma, a CT-guided biopsy was performed, which was non-diagnostic.
She was readmitted two weeks later with worsening pain. Her exam was benign other than abdominal tenderness to palpation. Labs showed a creatinine of 3.8 mg/dL (previous 1.0) and a hemoglobin of 9.8 g/dL. CT showed stable hydronephrosis and the ureteral stents were exchanged. She underwent exploratory laparotomy that showed a fibrotic, fixed retroperitoneal mass wrapped around the aorta that was biopsied. She was transferred to our institution before pathology results were available.
On arrival, ESR and CRP were 64 mm and 4.6 mg/dL, respectively. Repeat imaging showed plaque-like retroperitoneal soft tissue, encasing the aorta and IVC to the proximal common iliac vessels. Pathology from her intraoperative biopsy revealed dense fibrosis with scattered plasma cells, consistent with idiopathic retroperitoneal fibrosis. Nephrology consultation recommended initiating prednisone and Cellcept. At her post-discharge follow up appointment, her pain had improved, her creatinine was down to 0.8 mg/dL, and her CRP was <0.2 mg/dL.
Discussion:
Retroperitoneal fibrosis (RPF) is a rare condition characterized by inflammation and fibrosis in the infrarenal retroperitoneal space that can lead to ureteral obstruction. It is a form of periaortitis that is often idiopathic, but can be associated with malignancy, radiation, or certain medications. Patients typically present with abdominal or flank pain, weight loss, elevated inflammatory markers, anemia, and ureteral obstruction. Imaging typically shows a periaortic soft tissue density extending from the renal to the proximal iliac vessels with ureteral obstruction. Biopsy is not usually required for diagnosis. Treatment of the idiopathic form involves immunosuppression to reduce inflammation, reverse fibrosis, and urologic interventions to decompress the ureters. In this case, the patient’s treatment was delayed, resulting in multiple hospitalizations and exposure to numerous procedures and imaging studies. Her protracted course may be secondary to our unfamiliarity with this clinical condition and, thus, the delay in diagnosis.
Conclusions:
Idiopathic RPF is a rare condition of inflammation and fibrosis in the retroperitoneal space leading to ureteral obstruction and renal failure. If its clinical presentation goes unrecognized by the hospitalist, it could lead to unnecessary testing, procedures, consults, and delays in initiating immunosuppression and ureteral decompression.