Background: The timing and pace of patient discharges are not level-loaded throughout the day at many institutions including our own. At present, only 8% patients are discharged with rooms marked dirty by 11.00 am at our institution. To address this issue, we present the “Discharge when medically ready” model that has been implemented at our institution. The model was derived from the findings of a comprehensive, multidisciplinary needs assessment grounded in process improvement principles to help identify barriers and solutions to facilitate early discharges.
Purpose: To develop an improved interdisciplinary discharge readiness process that ensures safe and timely discharge once a patient is medically ready and supports our project goal of 25% of discharges and room marked dirty by 11.00 am.
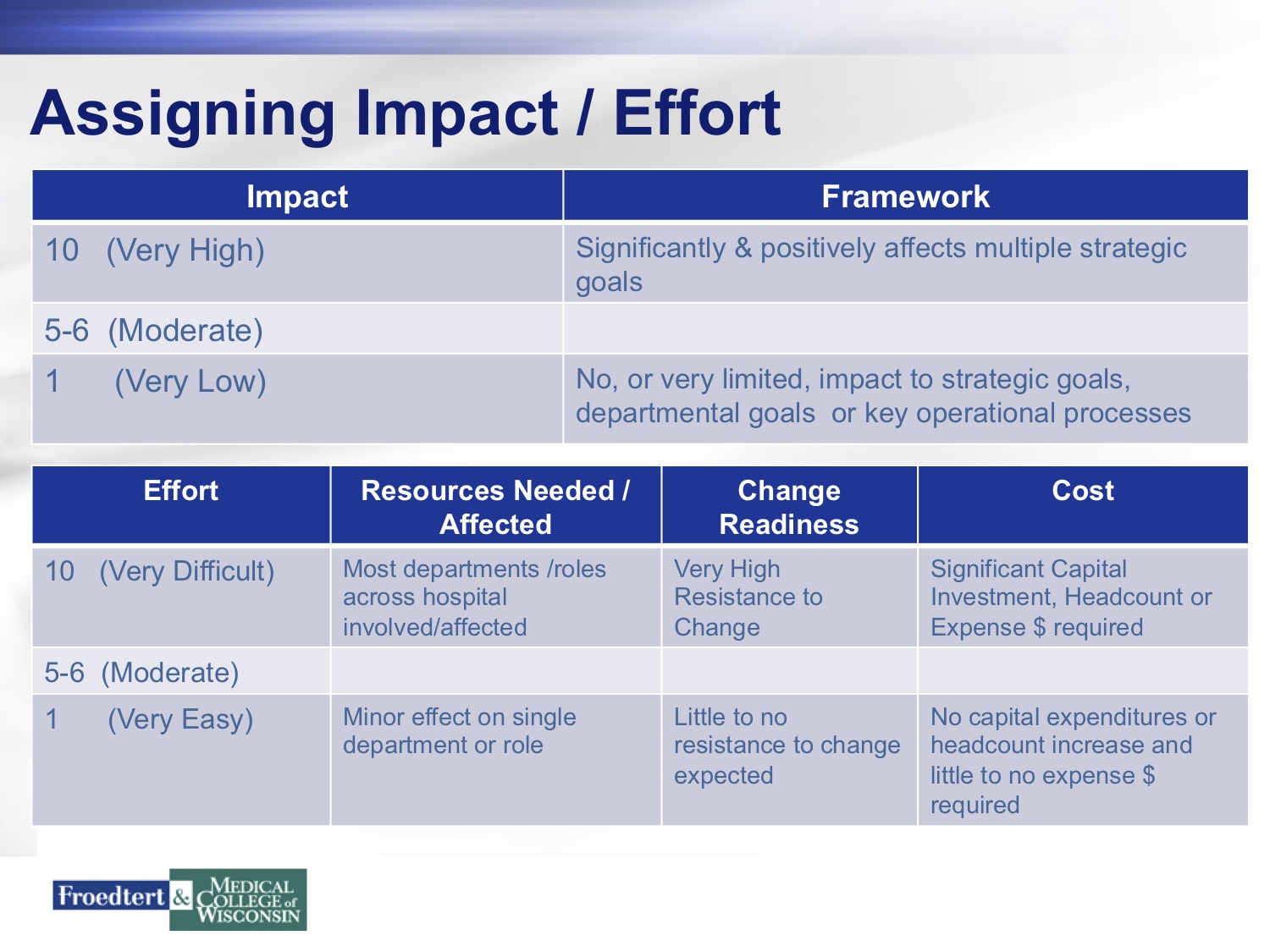
Description: We put together a multidisciplinary team including MD and APP providers, nursing, pharmacy, respiratory therapy, radiology administrators, laboratory technicians, physical and occupational therapists, speech therapists, environmental services, transport services, food and nutrition delivery, security and Electronic Health Record (EHR=EPIC) personnel. This team of 45 stakeholders met at least twice a month over the span of 8 months. Their input on the impact of intervnetions, effort needed, resources needed, change readiness and cost was used to identify high yield leverage points in our discharge process (see figure 1). Interventions with the highest score were incorporated into the “Discharge when medically ready” model.
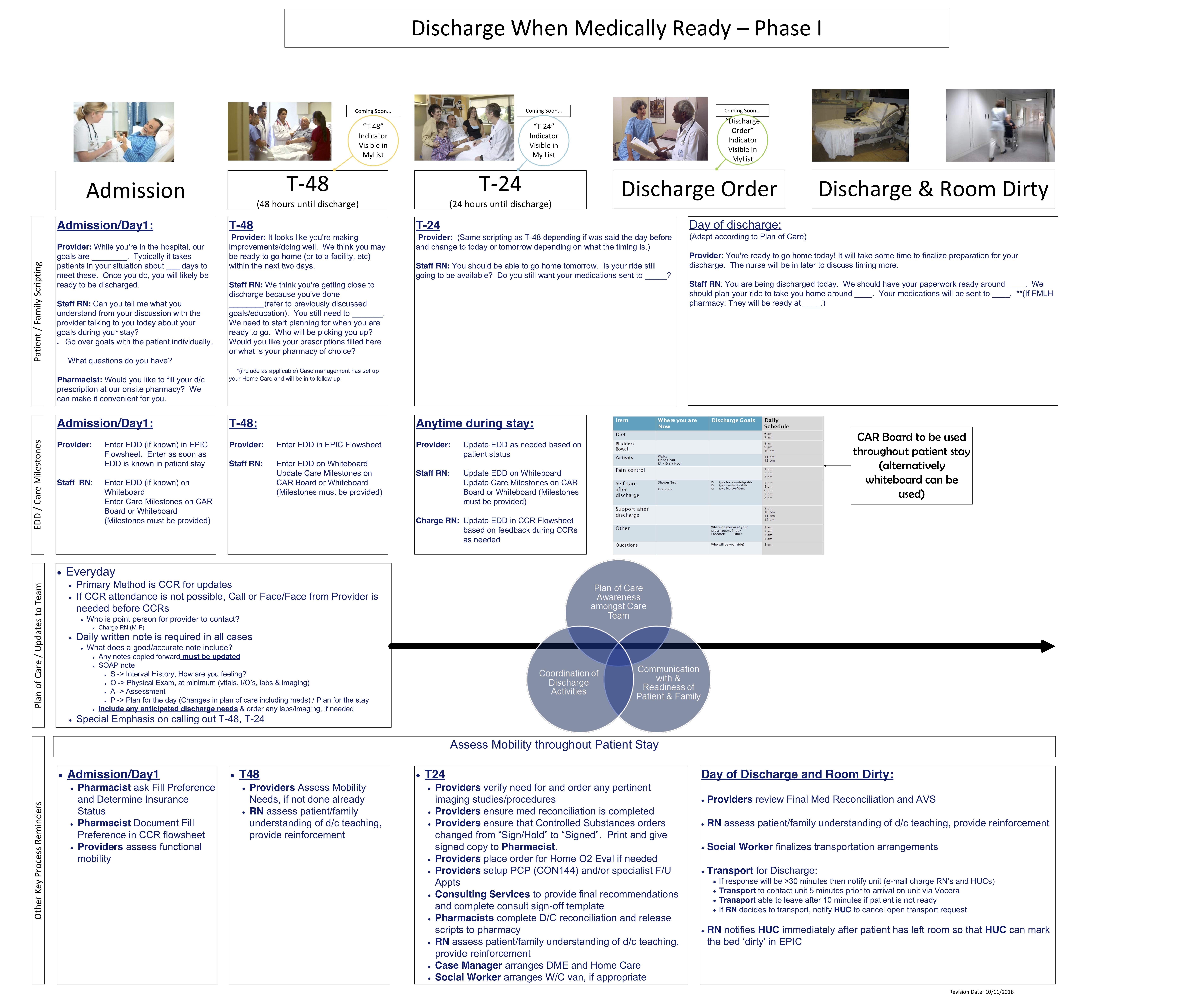
Multiple high impact and high feasibility interventions by various stakeholders have been identified to facilitate timely discharges. All stakeholders in the multidisciplinary team will itiretively perform key tasks to systematically facilitate a timely discharge. In addition to the day of admission and day of discharge, standard terminology identifying a patient’s discharge readiness has been implemented in the form of “T-48” (48 hours prior to discharge) and “T-24” (24 hours prior to discharge). This is visible to all members of the multidisciplinary team in the EHR as they work together to prepare the patient for discharge (see figure 2).
Conclusions: The three broad areas identified by our needs assessment include plan of care awareness amongst the care team, effective multidisciplinary coordination of discharge activities and dynamic communication with patient and family. The impact of this interdisciplinary discharge readiness process improvement on early discharges, readmission rates and length of stay will be assessed in the coming months.