Background: Mitochondrial disease (MD) refers to a group of clinically heterogeneous disorders that result from dysfunctional oxidative phosphorylation and subsequent cellular incapability to meet energy demands. Mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes (MELAS), myoclonus, epilepsy, ataxia with ragged red fibers (MERRFs), chronic progressive ophthalmoplegia, Kearns–Sayre syndrome, and sensory ataxia neuropathy dysarthria ophthalmoplegia are among several syndromes that have been associated with MD. However, with an estimated prevalence of 1 in 5000 people, previous studies about inpatient characteristics and clinical outcomes have been limited by the rare nature of MD. This study aimed to explore the relationship between MD and inpatient clinical outcomes.
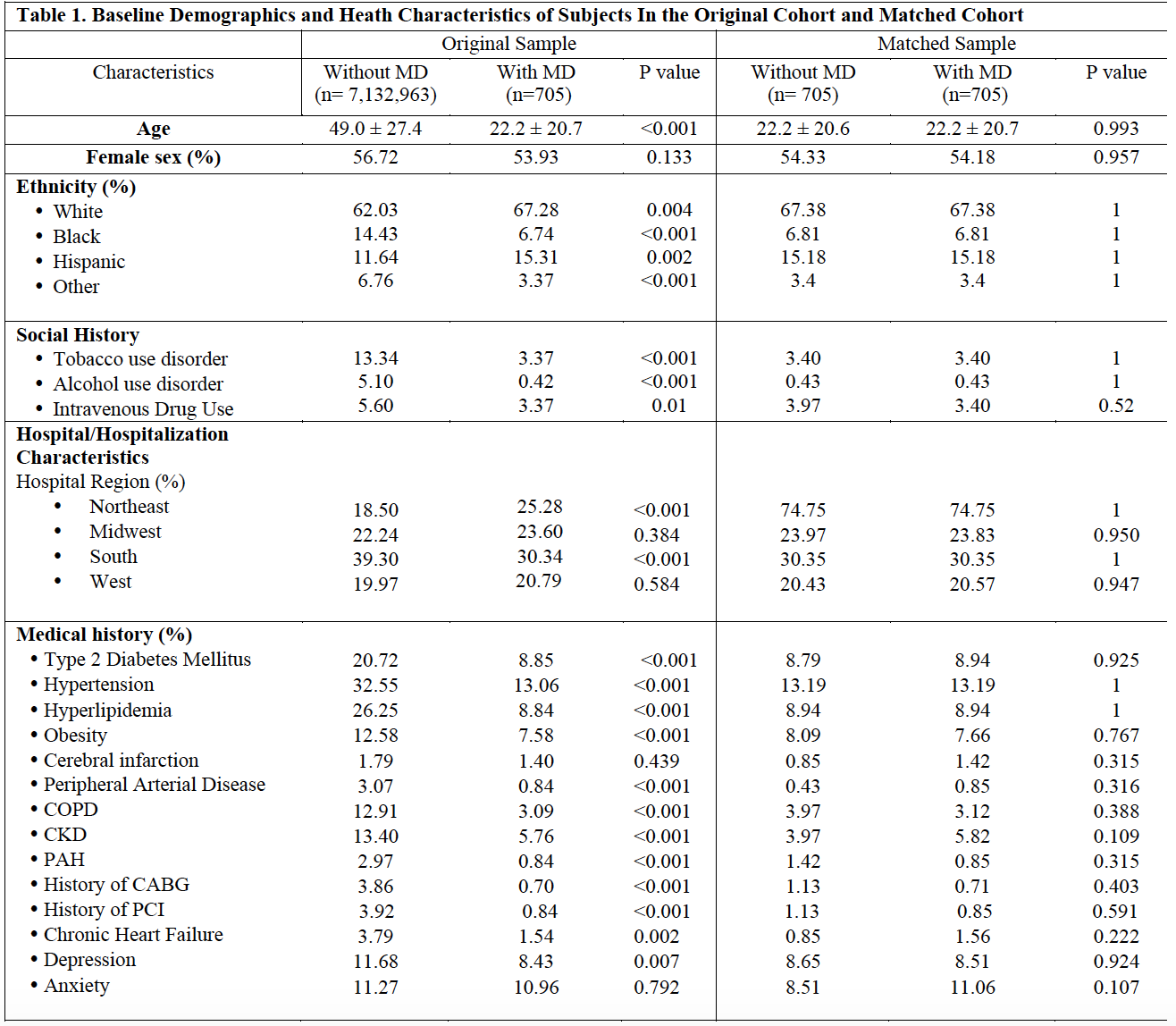
Methods: The 2016 National Inpatient Sample (NIS), which includes data from over 7 million subjects, was used for this study. Baseline demographics and clinical characteristics were compared between patients with MD (ICD9/10 codes 277.87/E88.4) versus patients without MD. Propensity scores were estimated from baseline patient characteristics and used to assemble a matched cohort to examine the impact of MD on major adverse cardiac events (MACE), including all-cause in-hospital mortality, cardiac arrest, and acute congestive heart failure (both systolic and diastolic) as well as sepsis, acute kidney injury (AKI) and need for mechanical ventilation.
Results: In total, 705 patients were identified with a diagnosis of MD. The mean age was 22 +/- 21 years with slightly more females (54%) than males and 67% Caucasian patients. MD, when compared to their matched cohort without MD, is associated with 2.4-fold increased odds of MACE (OR 2.42; 95% CI 1.29-4.57; p = 0.005) and more than doubled odds of systolic heart failure (OR 2.37; 95% CI 1.08-5.22; p = 0.027). In addition, MD is associated with 14-fold increased odds of all-cause in-hospital mortality (OR 14.22; 95% CI 1.87-108.50; p = 0.008). Patients with MD were more likely to have general diagnosis of heart failure (OR 1.75; 95% CI 1.01-3.03; p = 0.043), systolic heart failure (OR 2.37; 95% CI 1.08-5.22; p = 0.027), and cardiomyopathy (OR 4.10; 95% CI 2.10-8.01; p < 0.001). There were no significant differences in the rates of diastolic heart failure, cardiac shock, PCI, cardioversion, pacemaker, ICD, atrial fibrillation, atrial flutter and supraventricular tachycardia between two groups. In addition, MD was associated with increased odds of having AKI (OR 2.04; 95% CI 1.27-3.28; p = 0.003), sepsis (OR 8.33; 95% CI 2.93-23.69; p < 0.001), and receiving mechanical ventilation (OR 6.40; 95% CI 3.92-10.43; p <0.001).
Conclusions: To the best of our knowledge, this is the first study that examines a large database to characterize clinical manifestations of mitochondrial disease amongst inpatients in the United States. Mitochondrial disease is associated with a significantly increased risk of inpatient MACE, in‐hospital mortality, systolic heart failure, sepsis, and AKI.