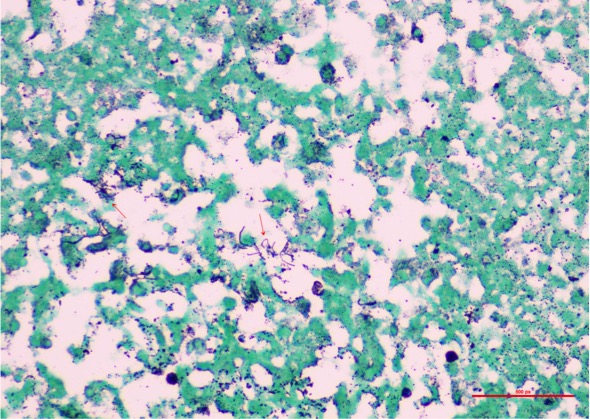
Case Presentation: A 78-year-old woman with severe persistent asthma on a maximum dose of inhaled corticosteroids (ICS) was admitted for lethargy and skin nodules on her thighs. She had three hospital admissions in the past two months for reported pneumonia. She was found to have fever, left basilar crackles, and multiple violaceous, firm, tender subcutaneous nodules on the abdomen and lower extremities. She had no leukocytosis, and blood cultures were negative. CT chest revealed a mass-like consolidation in the right lower lobe. Punch biopsies of the skin nodules initially revealed a suppurative process with lymphoplasmacytic cell infiltrate; gram and PAS stains failed to show any organism. The course of her admission was complicated by severe headache and worsening lethargy. Brain MRI revealed ring-enhancing lesions suggestive of abscesses. CSF cultures were negative. Further review of the skin pathology demonstrated few gram-positive filamentous organisms. The patient received TMP-SMX, Meropenem, and Linezolid for empiric coverage of actinomycetes, with interval resolution of lung and skin nodules, but worsening of mental status and brain lesions. She underwent craniotomy for evacuation of intracerebral abscess. Brain tissue grew Nocardia farcinica, which subsequently was isolated from all the sampled tissues. The patient’s mental status and functional capacity markedly improved, and she was discharged with a nine-month course of oral TMP-SMX and Linezolid. Follow-up neuroimaging revealed resolution of the abscesses.
Discussion: Disseminated nocardiosis is defined as involvement of two noncontiguous sites and is associated with a mortality rate as high as 64%. Lung seems to be the organ most frequently involved. The majority of cases of pulmonary or disseminated disease occur in people with deficient cell-mediated immunity, such as lymphoma, transplantation, chronic glucocorticoid therapy, and AIDS. To date, only several cases have been reported in patients with exposure to ICS as the only identifiable risk factor. ICS act by suppressing inflammation in asthma, and it is not surprising that the counter-effect would be increased susceptibility to infections. Alveolar macrophages are the resident phagocytes, which, along with T-cells, coordinate an immune response to clear the pathogen. However, Nocardia has enhanced resistance against intracellular killing. Therefore, clearance of such organisms relies heavily on the T-cell cytotoxic response, with a critical dependence on IL-12/IFN-gamma axis. Steroids, including ICS, have an effect on aforesaid pathways by inhibiting transcription of pro-inflammatory cytokines and by pro-apoptotic effects on T-cells. In a single center observational study, it was noted that the mean time to diagnosis of disseminated nocardiosis was 42 days. A high clinical suspicion is vital for an early diagnosis and appropriate treatment in patients who present with lung involvement or signs of non-resolving pneumonia. Our case illustrates the importance of considering ICS use, especially at maximum recommended dosage, as a risk factor for Nocardia infection.
Conclusions: ICS have an inhibitory effect on the T-cells involved in the production of cellular immunity. Hence, they can cause sufficient immunosuppression to predispose a patient to disseminated infections with intracellular organisms, such as Nocardia.