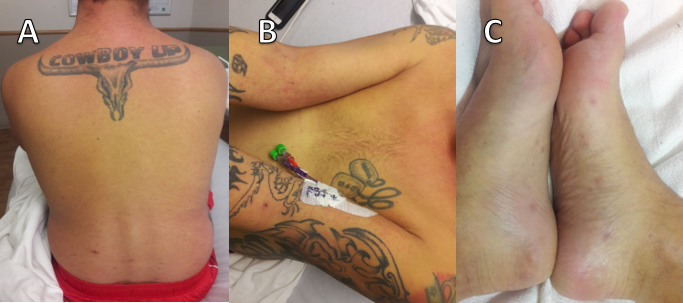
Case Presentation: A 31-year-old man presented to the ED with one week of worsening cough, headaches, and abdominal pain. Initial laboratory evaluation revealed a total bilirubin level of 15.6 mg/dL, ALP 181 U/L, ALT 518 U/L, AST 829 U/L. Lipase and GGT were within normal range. Chest x-ray and abdominal ultrasound showed no abnormalities. He had a 13 pack-year smoking history but no alcohol use. His urine drug screen was negative, and acetaminophen level was undetectable. No recent travel history or new sexual partners within the last 2 years. No family history of autoimmune or liver disease. On examination, he was jaundiced with RUQ tenderness and hepatomegaly. Further investigations confirmed vaccination against hepatitis A and B. Viral studies for hepatitis C, HIV, EBV, CMV, ADV, and VZV were negative. An HSV IgM was positive, while IgG was negative. Rheumatologic testing was positive for ANA (1:640) and AMA. Due to the positive HSV IgM, he was given 900mg IV acyclovir every 8 hours for possible HSV hepatitis. Despite the treatment, his bilirubin and transaminases continued to rise.On day six, he developed a maculopapular rash over the trunk, back, and extremities including his palms and soles (Figure 1). Testing for syphilis revealed a positive RPR titer and a reactive treponemal antibody test. One dose of 2.4 MU of penicillin G benzathine was administered. Liver biopsy was obtained the next day which showed portal and lobular hepatitis and hepatocyte necrosis. HSV-1 and HSV-2 immunohistochemical stains were non-reactive, and spirochetes were not visible on Steiner stain. Following penicillin administration, transaminases trended downwards and he reported profound symptomatic improvement.
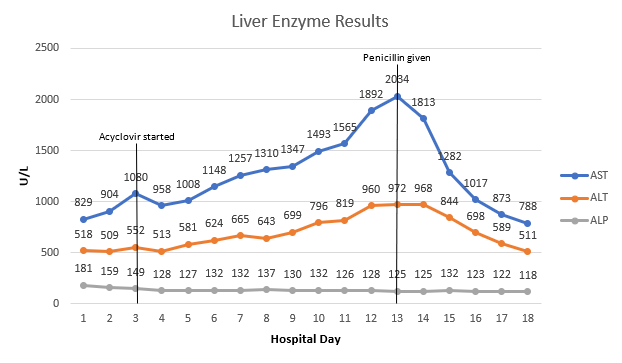
Discussion: Syphilis is often considered in the context of painless genital ulcers, lymphadenopathy, and cutaneous manifestations in sexually-high-risk populations. Hepatitis is an uncommon manifestation of syphilis. Laboratory findings typically follow a cholestatic pattern with marked elevations in ALP and GGT and milder elevations in aminotransferases.1–3 This case is remarkable due to mild ALP elevations and impressive elevations in AST and ALT. Several possible diagnoses competed before testing for syphilis occurred, including HSV hepatitis. In this case, transaminitis continued to worsen until penicillin was administered (Figure 2). There is evidence that both ANA and AMA can be falsely positive in patients with bacterial infections, including syphilis.4,5 The diagnosis of syphilitic hepatitis was made based on the dramatic clinical and laboratory improvement seen after penicillin administration. Moreover, the biopsy findings in this case were consistent with a systematic review of 55 liver biopsies taken from patients with syphilitic hepatitis.1
Conclusions: • Syphilis should be suspected as a possible cause in patients with acute hepatitis and jaundice.• Liver enzymes can be markedly elevated in syphilitic hepatitis with mild increases in ALP.• False positive serology testing can occur in syphilis.