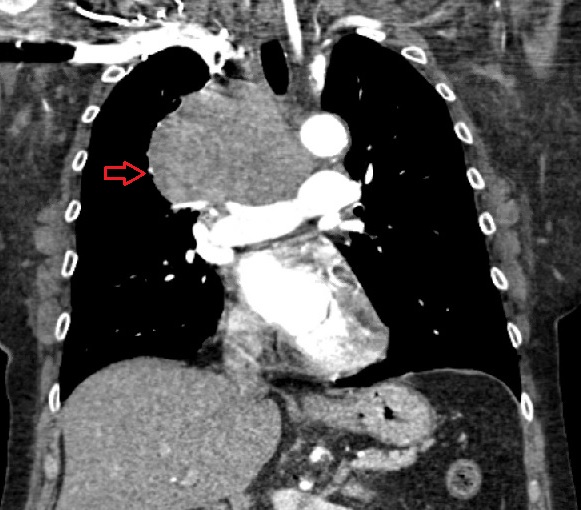
Case Presentation: A 59 year-old female with past medical history significant for chronic hyponatremia and tobacco use presented to the hospital with complaints of dyspnea and neck pain for 2 weeks. She reported blurry vision and swelling in her neck, face and axillae. Initial vitals were stable. Admission labs were significant for sodium 125, baseline for 10-months. On examination, there was facial plethora, palpable anterior cervical lymphadenopathy, facial and neck swelling with visible distension of neck veins and upper abdominal vein distension. CT chest showed a 7x9x7 cm multi-lobulated anterior mediastinal mass compressing the superior vena cava (SVC) causing severe stenosis. SVC syndrome was evident. Biopsy of the mediastinal mass demonstrated SCLC. Further imaging ruled out metastasis. Emergent radiation therapy with eventual high dose steroid was initiated with significant clinical improvement. After completing radiation treatments, cisplatin and etoposide was initiated with oncologic follow up. Regarding patient’s chronic hyponatremia, she was hospitalized 10 months prior for a sodium level of 111. Pertinent workup met criteria for diagnosis of SIADH and CT chest during that admission was negative for any acute process.
Discussion: We present an unusual case of a patient with SIADH 10-months prior to the diagnosis of lung cancer. Lung cancer constitutes 13% of all new cancer diagnoses, making it the second most common malignancy and the deadliest in the United States. Small cell lung cancer (SCLC) makes up 15% of lung cancers, where hyponatremia is frequently related to syndrome of inappropriate antidiuretic hormone (SIADH). Neoplastic syndromes are involved in approximately 10% of SCLC cases. Among the paraneoplastic syndromes, SIADH is the most prevalent at 40%. Lung cancers presenting as a paraneoplastic syndrome have no associations with size or stage of primary lung malignancy.
Conclusions: We describe a rare case of SIADH manifesting as a precursor to SCLC complicated by SVC syndrome. Given this patient’s chronic hyponatremia and prior negative imaging, her clinical course is suggestive of antidiuretic hormone secretion by the malignancy before it was clinically detected. This case serves as a reminder to recognize subtle changes, such as worsening dyspnea in patients with SIADH to have a lower threshold for re-image. Additionally, hyponatremia may be a marker of occult malignancy, which merits attention for cancer screening with appropriate serial imaging. Such recommendations require further research of antidiuretic hormone levels and hyponatremia in correlation to early detection of SCLC. This can provide guidelines for cancer surveillance programs and potentially improve malignancy survival rates.