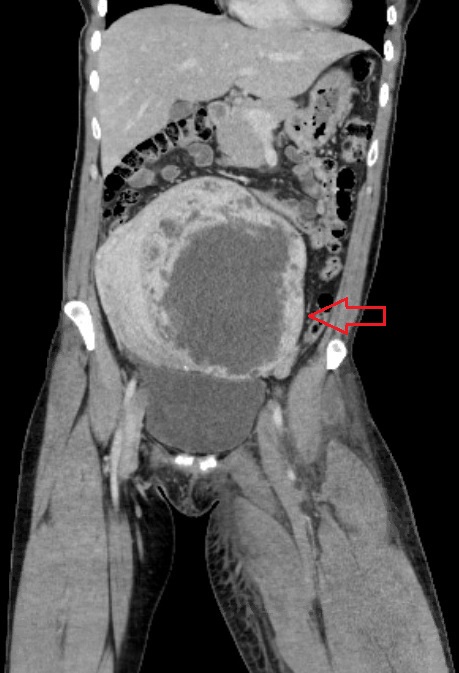
Case Presentation: A 46-year-old previously healthy female, presented to the hospital for left leg pain and swelling. She was febrile and tachycardic. Examination showed abdominal distension with a palpable firm, nontender lower abdominal mass, left lower extremity tenderness, nonpitting edema extending to upper thigh, mottled skin, and diminished pulses. Doppler showed totally occluded DVT of common femoral vein extending to posterior tibial vein. Patient was started on therapeutic anticoagulation. CT abdomen revealed a large heterogeneous uterine mass measuring 18.6×15.5×9.9 cm, causing mass effect and a left common iliac vein thrombus extending into the external and internal iliac veins. She was taken for transcatheter thrombolysis and mechanical thrombectomy. Post-intervention she was found to have increased leg pain and swelling. Subsequent venogram showed recurrent DVT. Surgical intervention of uterine mass was planned. Patient underwent successful hysterectomy and another mechanical thrombectomy with stent placement into common iliac vein. A final venogram demonstrated no significant residual thrombus with adequate flow. Uterine mass pathology resulted as fibroid. Patient was continued on oral anticoagulation and stable for discharge.
Discussion: The urgency for diagnosis and treatment is critical as we described an unusual presentation for May-Thurner syndrome (MTS) in the setting of uterine fibroids. MTS is an uncommonly diagnosed anatomic pathology causing deep vein thrombosis (DVT), which develops during compression of the left iliac vein by the right iliac artery against the lumbar spine. This leads to extensive thrombotic occlusion of major and collateral veins, which backs up into arterial vasculature, also known as phlegmasia cerulea dolens. Increased pressure within the extremity causes limb cyanosis, paresthesia, motor weakness and eventual critical limb ischemia. Multiple risk factors are known to cause MTS, such as, third-trimester pregnancy, dehydration, and pelvic masses.
Conclusions: MTS is underdiagnosed possibly due to the more recognizable risk factors for DVT which are easily identified. Uterine fibroids causing MTS is rarely diagnosed but prevalent in postmortem cases. Urgent intervention with thrombolysis is imperative for salvage of a critical limb in MTS. Although it is not recommended in all cases of MTS, endovascular stent placement does improve symptoms and increases vasculature patency rates. This case highlights the unusual presentation of MTS by uterine fibroids with successful treatment by total abdominal hysterectomy, thrombolysis, mechanical thrombectomy, and endovascular stenting.