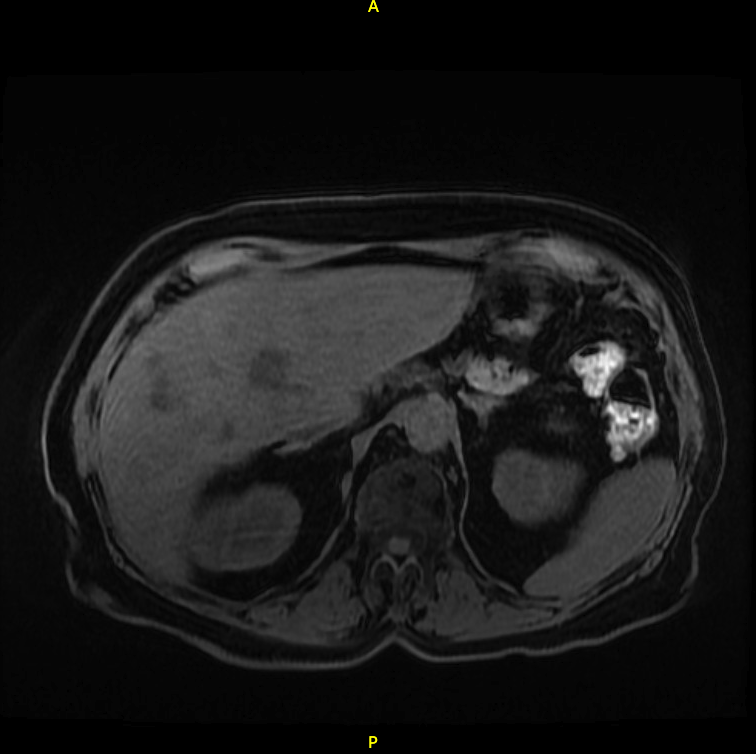
Case Presentation: A 78-year-old female with a history of CAD, hypertension, and asthma presented to the ED with fatigue, abdominal pain, diarrhea, and decreased urine output for three days. She recently returned from Southern France where she had overexerted herself in the heat. She was ill-appearing. Vital signs and exam were normal. Significant labs/imaging: Na = 125 mmol/L, CO2 = 14 mmol/L, BUN = 79 mg/dL, Cr = 8.3 mg/dL, WBC = 17.40 10^9/L, HGB = 10.6 g/dL, Alk Phos = 217 IU/L, AST = 128 IU/L, ALT 101 = IU/L, bilirubin = 0.5 mg/dL. CT abdomen/pelvis revealed sigmoid wall-thickening and liver abscesses. She became anuric and was started on emergent hemodialysis. The liver abscess was drained. Cultures of blood and liver abscess fluid grew streptococcus intermedius. Her ECHO was negative for any vegetation. Renal biopsy revealed acute AIN. Of note, she had a normal colonoscopy 2 years ago.She was started on IV ceftriaxone, metronidazole, and steroids. Other extensive infectious workup, hepatitis panel, and autoimmune panel were negative. She remained on hemodialysis without any renal recovery. She clinically improved and was eventually discharged on two weeks of oral cefuroxime 100 mg daily and metronidazole 500 mg TID. She continued dialysis and followed up with the infectious disease. An outpatient colonoscopy to rule out colon cancer was also scheduled.
Discussion: Streptococcus intermedius (of the Streptococcus anginosus group) is an infrequent pathogen, but part of normal flora of the oropharynx, genitourinary and gastrointestinal tracts with a propensity to cause suppurative infection. Strep intermedius bacteremia should raise suspicion for colon cancer. Infection-related AIN is managed by treating the underlying infection; the role of steroids is unclear. High metabolic demand and decreased blood supply make the tubulointerstitium more susceptible to injury. This case posed a challenge given the uncommon etiology and rapid progression of renal failure. Infection-associated AIN is underdiagnosed; this patient’s progression to ESRD despite treatment highlights the importance of a high index of suspicion.
Conclusions: We report a case of an immunocompetent patient, who developed Streptococcus intermedius bacteremia, multiple liver abscesses, and acute interstitial nephritis (AIN), which progressed to end-stage renal disease (ESRD) requiring hemodialysis.