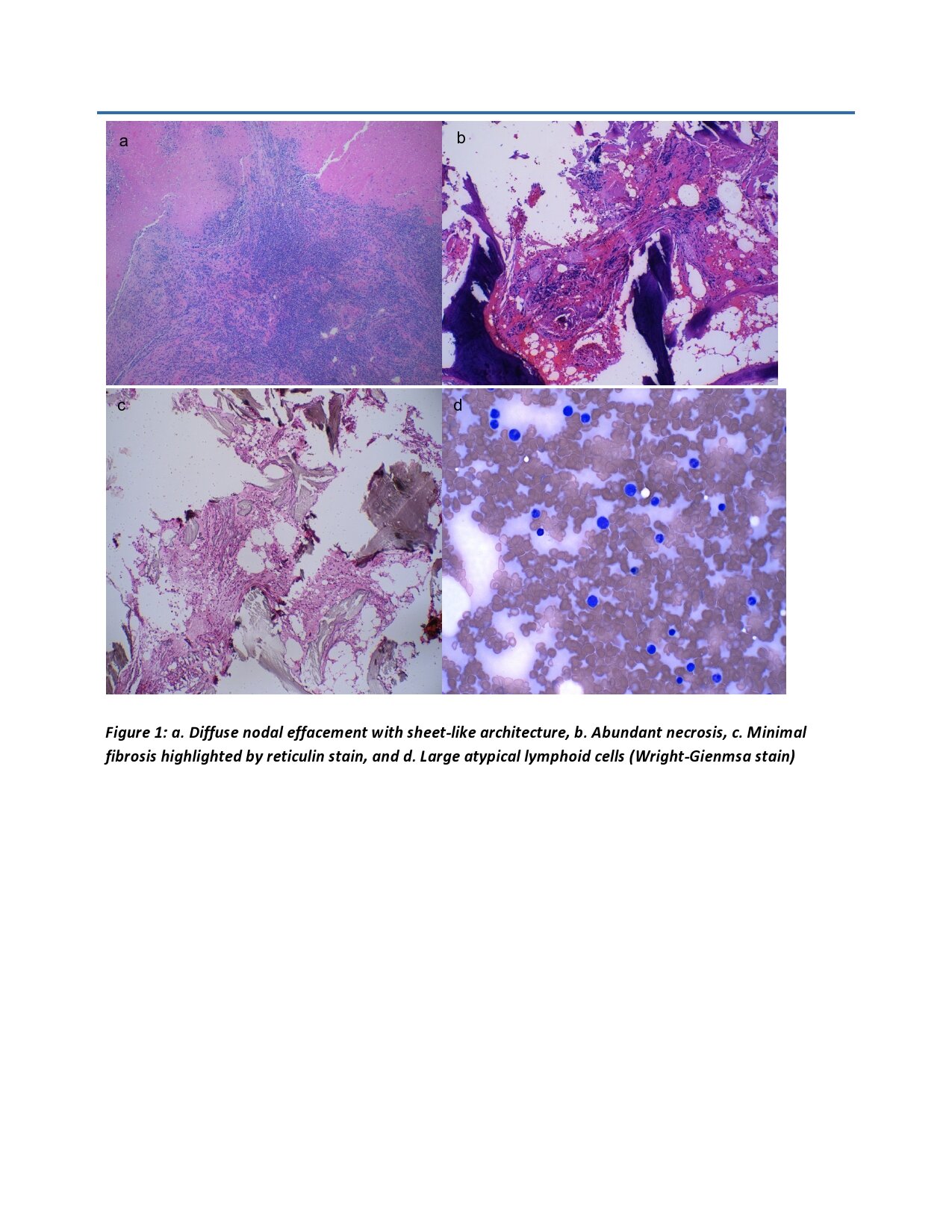
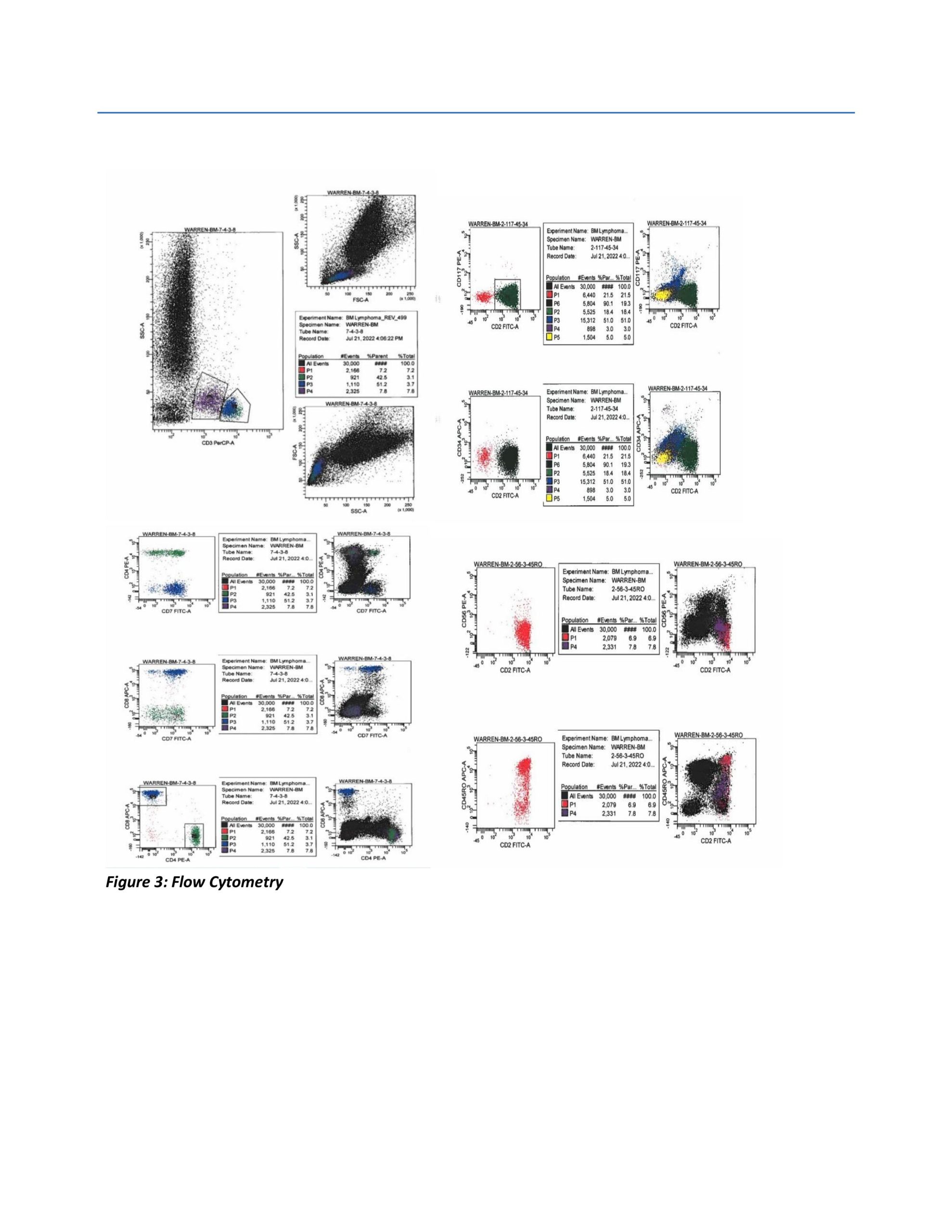
Case Presentation: Our patient is an 83 year old female with medical history of right breast cancer treated with lumpectomy and chemo-radiation 12 years ago. She presented with complaints of generalized weakness and confusion for 5 days. On admission, labs were significant for elevated calcium level of 17.2 mg/dL, white blood cell count (WBC) of 15100/uL, and low Vitamin D levels. She was started on aggressive intravenous hydration and was given calcitonin. Patient was subsequently treated with cinacalcet, prednisone and denosumab for recalcitrant hypercalcemia. Additional labs revealed elevated parathyroid hormone related peptide.. An initial diagnosis of paraneoplastic syndrome induced hypercalcemia was made. A Pan CT scan revealed diffuse lymphadenopathy and lymph node biopsy showed CD30-negative T-cell lymphoma. Patient was treated for hypercalcemia initially with Calcitonin and, Zomata, which was not able to bring calcium down to normal level. Concurrently chemotherapy was started for T-Cell lymphoma with cyclophosphamide, doxorubicine hydrochloride, vincristine and prednisone. The patient responded well to chemotherapy and her blood calcium level decreased dramatically after treatment. The patient was discharged home with outpatient chemotherapy.
Discussion: The median age of presentation of T-cell lymphoma is around 60 years. Patients often present with B symptoms such as weight loss, fevers, night sweats, fatigue, and generalized pain. Skin, gastrointestinal, lung, brain and salivary gland are a few of the extranodal sites that have been reported. Hypercalcemia is an uncommon presentation of lymphoma and is associated with a poor overall survival. Despite aggressive treatment, the prognosis for long term survival remains grim. A hypercalcemia associated with malignancy is a common lab finding usually present in patients with advanced stage malignancies. The major systems affected by hypercalcemia include neuropsychiatric, renal and gastrointestinal tract. Therefore these patients have severe hypercalcemia development over shorter periods leading to more severe presentations than other etiologies of hypercalcemia. The standard treatment for hypercalcemia associated with malignancy continues to be hydration with isotonic fluids at a high rate. Intravenous zoledronic acid is considered the first line in clinical settings whereas subcutaneous denosumab is clinically preferred in bisphosphonate resistant hypercalcemia and in cases of associated renal failure. Calcitonin either subcutaneous or intramuscular is recommended for short-term management along with hydration and bisphosphonate therapy. Patients with refractory hypercalcemia who are unable to tolerate intravenous hydration due to cardio-renal comorbidities should be considered for renal replacement therapy.
Conclusions: The T-cell lymphomas are a type of blood malignancy which are aggressive and rarely reported after being exposed to ionizing radiations which is part of a treatment therapy for different types of malignancies. Ionizing radiations cause lymphocytosis which leads to development of lymphomas. Hypercalcemia of malignancy is an endocrinology emergency and an early treatment is necessary to prevent complications. An aggressive treatment with IV fluids along with calcitonin and denosumab. Treatment of underlying malignancy is essential for the management of hypercalcemia.