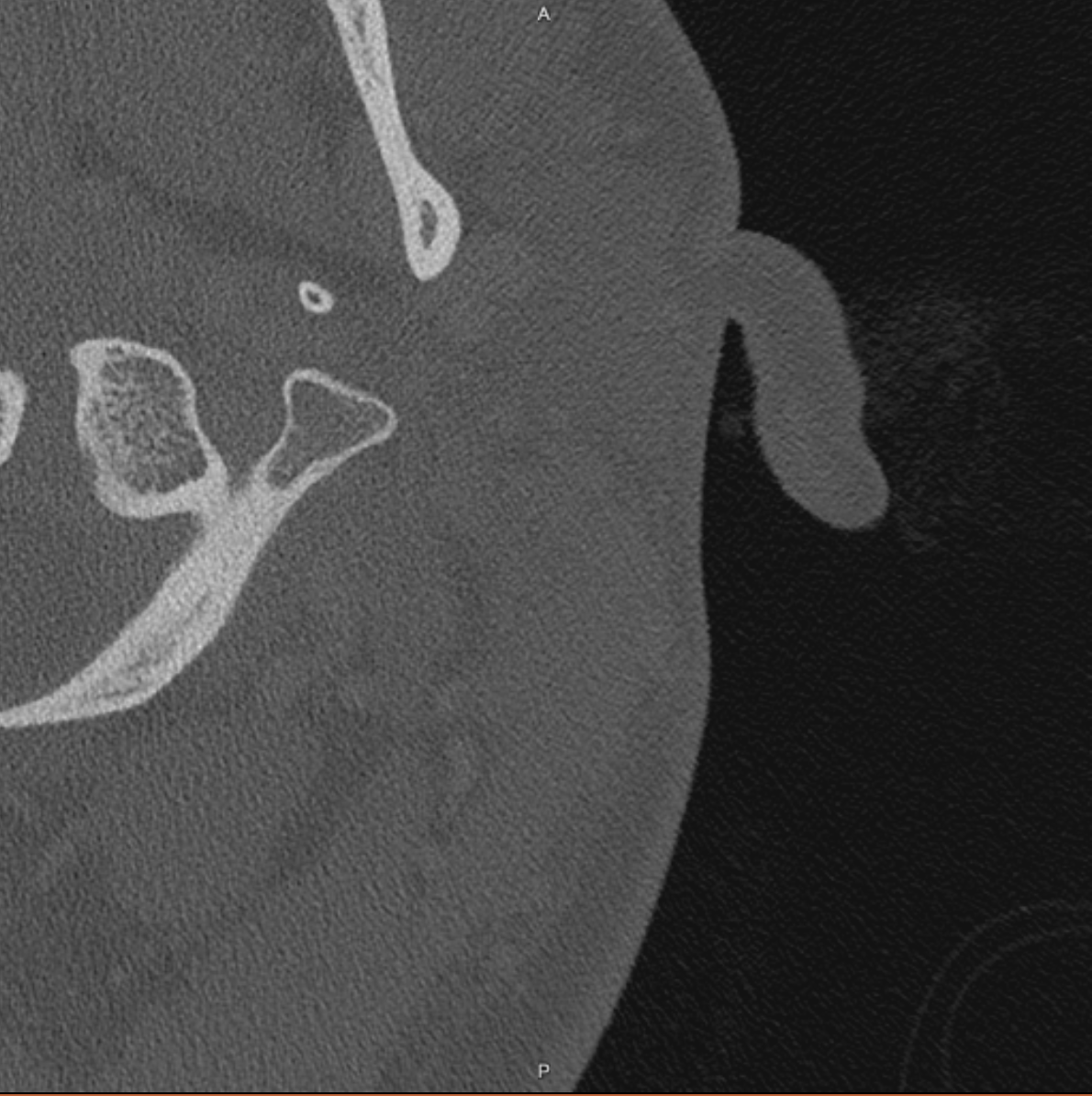
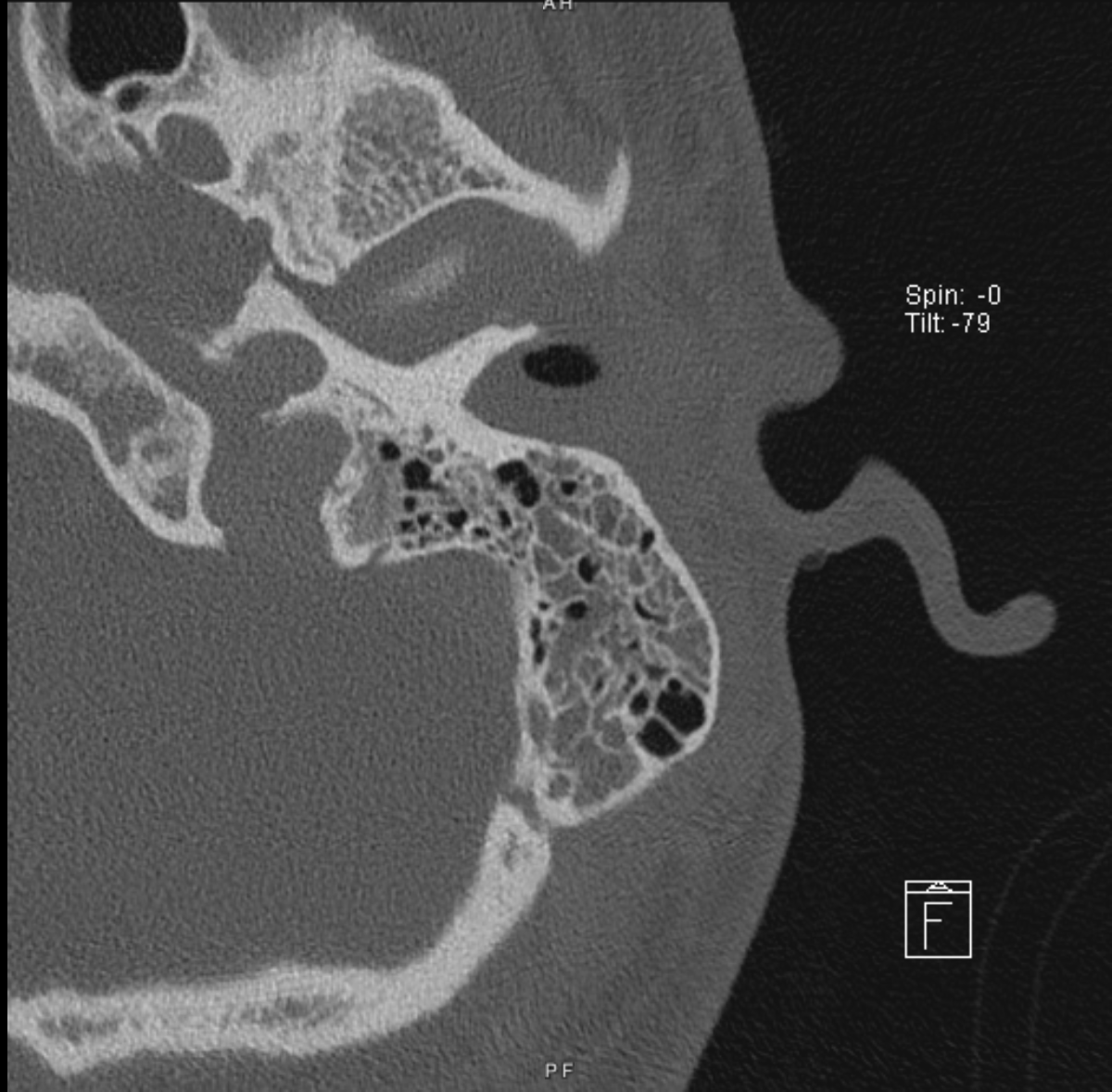
Case Presentation: A 19-year-old Mennonite male without significant past medical history who had not received any childhood vaccinations presented to the emergency department with left ear pain and neck rigidity for one week. The patient had a fever of 101°F with mastoid tenderness and left tympanic membrane rupture on physical exam. Computed tomography scan was ordered due to duration of symptoms and clinical suspicion of mastoiditis and revealed near complete opacification of the left mastoid, middle ear, and external auditory ear canal with two small areas of bone erosion indicative of left mastoiditis. The patient underwent emergent mastoidectomy and myringotomy with tympanostomy placement and received intravenous broad spectrum antibiotics with gram positive coverage. Intra-operative cultures of the ear discharge grew Streptococcus pyogenes susceptible to Ceftriaxone. A peripherally inserted central catheter line was placed and the patient was discharged with outpatient parenteral antimicrobial therapy for 6 weeks and Ear Nose Throat follow up.
Discussion: Acute mastoiditis is a rare nonmeningeal complication of otitis media1. It is a medical emergency requiring prompt diagnosis and treatment2. Unvaccinated status can lead to more severe infection. Although acute otitis media is one of the most common childhood bacterial infections, rates have declined with the pneumococcal vaccine3. Despite the patient’s culture growing a strain of Streptococcus that is not vaccinated against routinely in childhood, his unvaccinated status raised suspicion for mastoiditis and prompted further workup. Acute mastoiditis occurs due to extension of infection from the middle ear to the mastoid air cells, apart of the temporal bone4. Acute inflammation of the mastoid process leads to bony septation erosion5 . Clinical findings include fever, postauricular swelling, tenderness of ear pinna, severe otalgia, and ear drainage1. Although mastoiditis is a clinical diagnosis, radiologic imaging is used to support the diagnosis5. Diffuse opacification of the middle ears and mastoid air cells on CT confirms the diagnosis6. The most common causative agents are gram positive cocci5. Treatment involves broad spectrum antibiotics and myringotomy for culture and drainage1. If clinical status does not change after IV antibiotics or there are clear signs of osseous necrolysis on imaging, indicating severe infection, a mastoidectomy must be performed5. Intraoperative cultures guide antibiotic therapy5. Opportunistic infection can spread toward the brain or periphery due to the location of the mastoid process4. Complications involve encroachments of inflammation on neighboring structures in which case a tomography is indicated5. Left untreated, mastoiditis can lead to life-threatening sequela of subperiosteal abscess, meningitis, intracranial abscess, and venous sinus thrombosis4.
Conclusions: Acute mastoiditis is a rare complication of otitis media that presents with erythematous and edematous swelling of the mastoid process. Due to the widespread availability of childhood vaccinations, mastoiditis is often not a top differential diagnosis. Although it can be diagnosed clinically, CT scan is often used to confirm this can’t miss diagnosis. Treatment includes systemic antibiotics and if severe enough, mastoidectomy. Progression of acute mastoiditis can result in devastating, potentially life-threatening consequences making a prompt and accurate diagnosis critical.