Background: Clinicians face an overwhelming volume of communication through various channels, including phone calls, text messages, emails, in-person interruptions, and secure messaging systems. This information overload is increasing[1] and poses significant challenges. Despite the availability of communication tools, failures in communication remain the leading cause of preventable medical errors [2]. Secure messaging systems, while essential, create interruptions that disrupt workflow, increase cognitive load, and are associated with medical errors [3,4]. Interruptions reduce task accuracy by 44–80% [5]. This study quantifies the interruption burden of secure messaging and examines how it varies by clinical role.
Methods: We conducted a 2 week retrospective analysis of secure messaging at a quaternary, 880-bed hospital using a platform external to the electronic health record (EHR) from January 30–February 12, 2023, corresponding to a standard service block. Messaging frequency on general medicine (GM), specialty medicine (SM), and ICU teams with an attending + trainee or APP model were included. Service schedules were used to match message logs to clinicians on service, excluding days off, and days with three or fewer messages. Interruption intervals were calculated assuming an average 12-hour shift; weekend data was excluded.
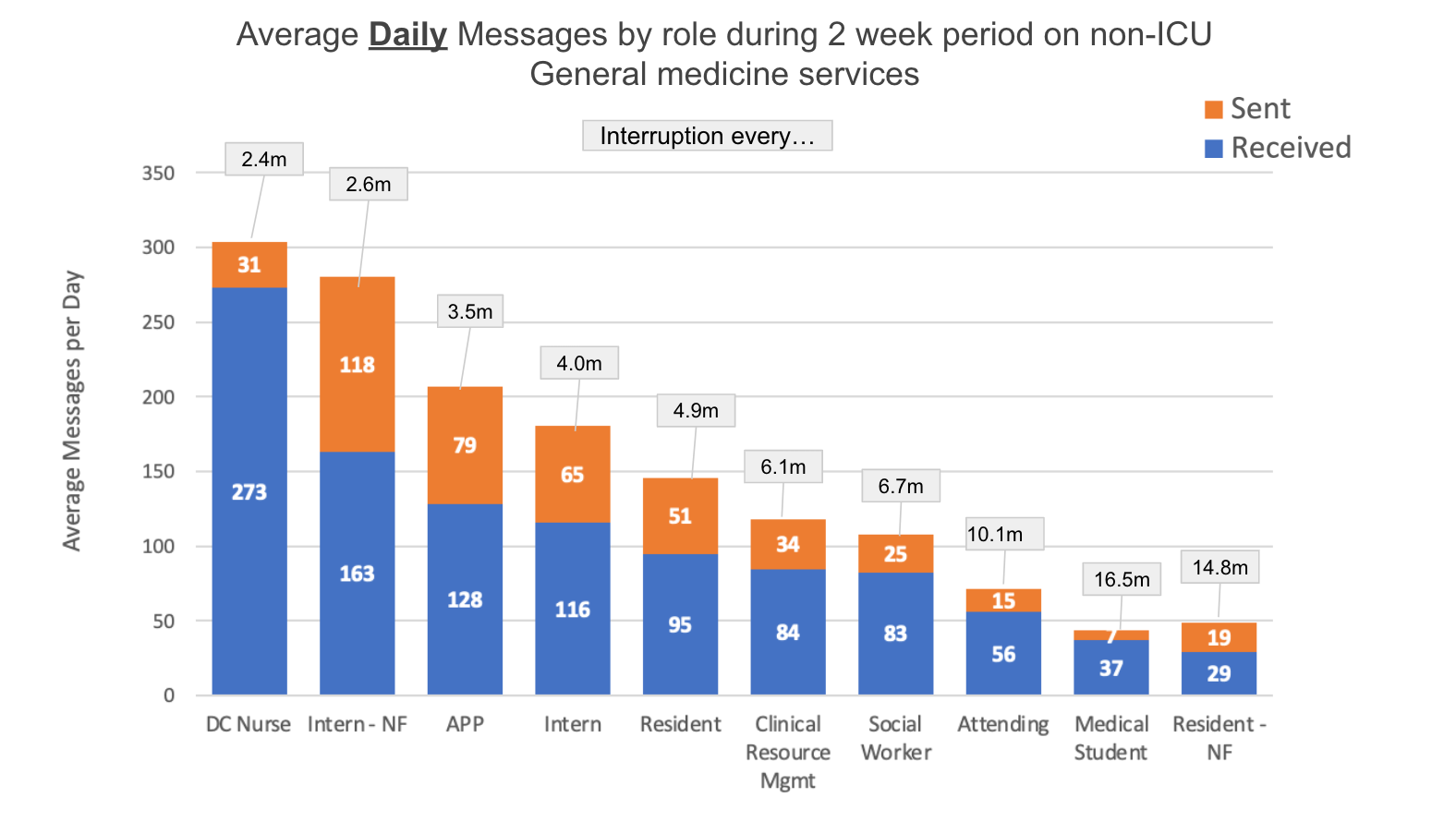
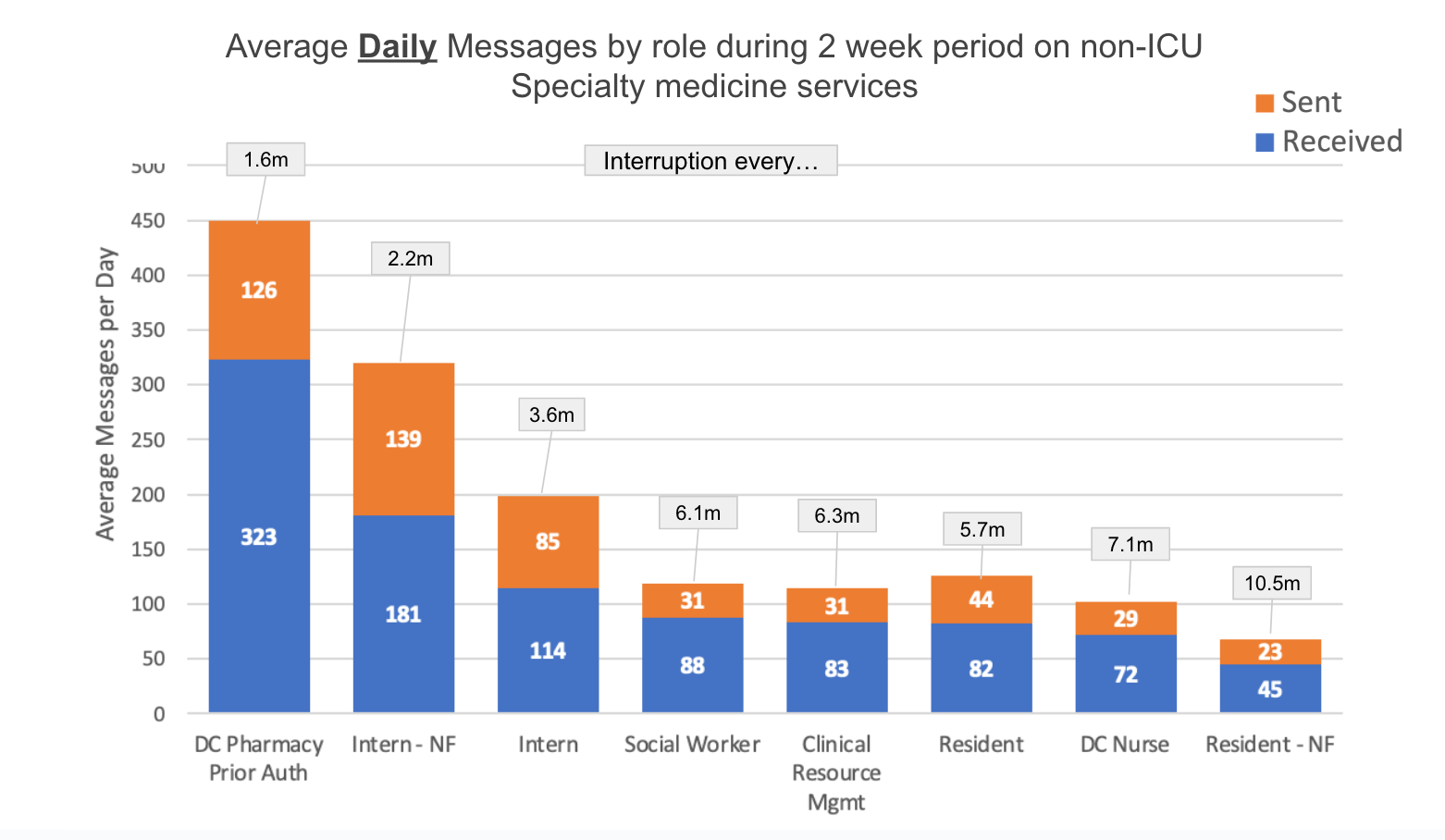
Results: During the study, 628,162 messages were sent, and 1,511,429 messages were read, averaging 62,816 messages sent per weekday. Each message sent created 3.4 interruptions. On GM (Fig 1) and SM (Fig 2) services, frontline clinicians were interrupted every 2.2-4 minutes (min), day residents every 4.9-5.7 min, and attendings every 10.1 min (SM attending schedules unavailable). Nurses were interrupted every 6.1-7.2 min, with rates likely higher for 8-hour shifts. Discharge coordination roles faced interruptions as frequently as every 1.6-7.1 min. Interdisciplinary ICU teams had lower rates with APPs interrupted every 8.3 min, day interns every 8.6 min, and residents every 10.5 min.
Conclusions: While secure messaging is a vital communication tool, it also significantly contributes to interruptions, averaging 3.4 per each message sent. During a 12-hour shift, interruptions occurred as frequently as every 1.6-14.8 min, increasing cognitive load, task accuracy, and risking patient safety. This level of disruption increases cognitive load, reduces task accuracy, and poses risks to patient safety. While prior studies have suggested improvements to messaging platforms, these efforts may primarily address the symptoms of the issue rather than the underlying problem. The high reliance on interruptive, immediate messaging could suggest a need to shift focus toward reducing the overall volume of messages, and instead develop a more strategic communication approach. We propose that organizations should consider critically evaluating what information is communicated, to whom, and when, and explore tools that support non-interruptive, asynchronous workflows, such as shared collaborative lists. These strategies could complement current efforts to improve messaging systems and help reduce interruption burden. This two-week analysis provides foundational data but is limited by the absence of census information, the short timeframe, and the single-site focus. Future studies should evaluate additional timeframes, other secure messaging systems, and multiple institutions.