Background: The decision to reinitiate anticoagulation after a trauma admission is complex. There have been limited studies on post-discharge outcomes of patients who are restarted on therapeutic anticoagulation after traumatic injury versus those who have had anticoagulation discontinued.
Methods: All consecutive patients on anticoagulants who were admitted to Saint Marys Hospital in Rochester, Minnesota for trauma between January 1, 2012 and December 31, 2021 were identified in the Mayo Clinic Trauma Registry. Data were collected via retrospective chart review and abstracted into REDCap© software. Patient characteristics upon admission and discharge and 1-year post-discharge outcomes were extracted. Discharged patients were categorized into two groups: Anticoagulation (AC) and No Anticoagulation (No AC) prescribed at discharge. Data were analyzed with SAS software (version 9.4; SAS Institute).
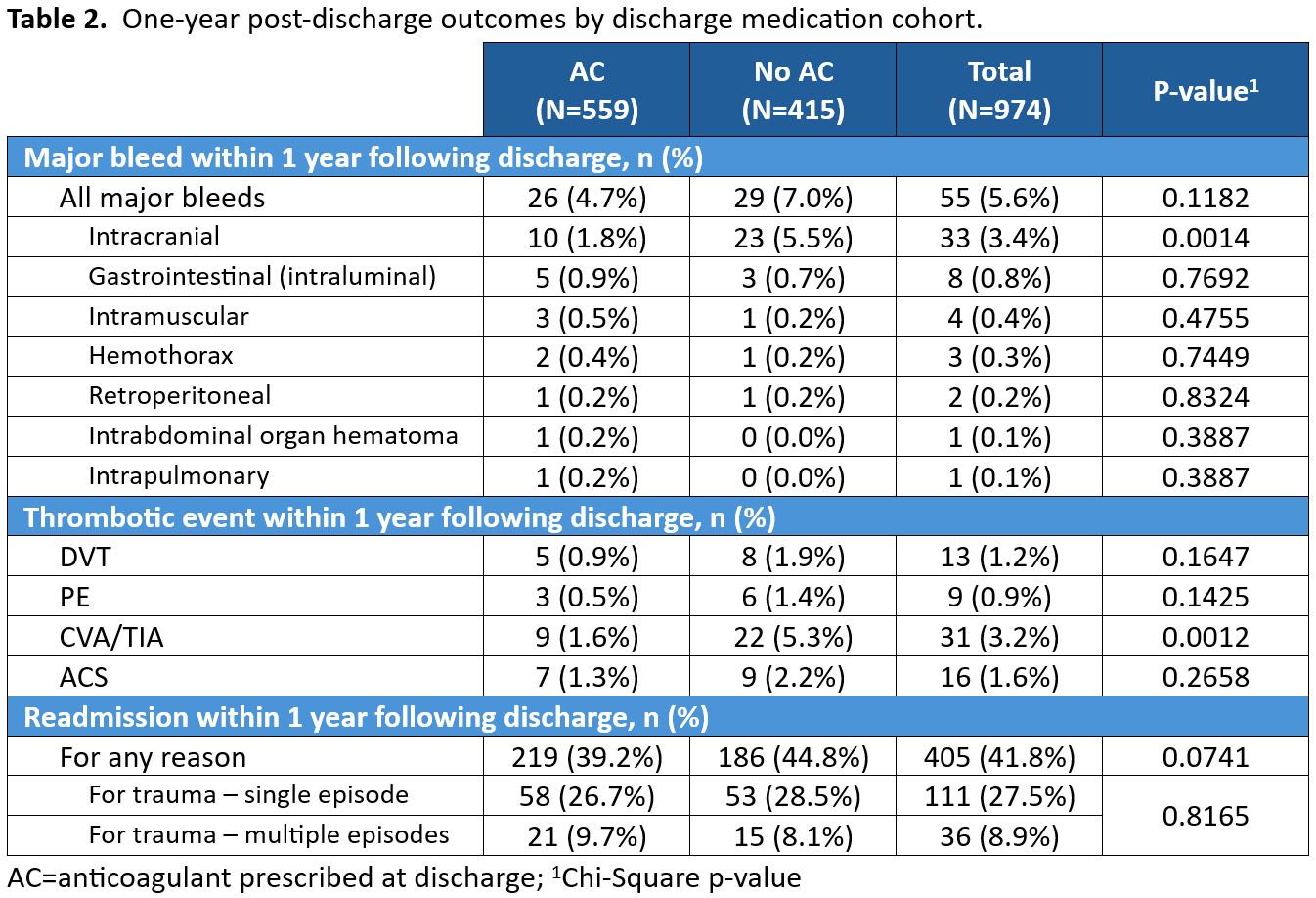
Results: A total of 1056 patients were on an anticoagulant at the time of hospital admission for trauma. The mean age was 77.4 years (+/-12.3 years), and 45% were women. The indication for anticoagulation in most patients was atrial fibrillation (70.9%). Most patients were prescribed warfarin (81.7%), followed by direct oral anticoagulants (16.5%) and heparins (1.8%). There were 974 patients who survived hospital admission to discharge. Of these patients, 559 were discharged on an anticoagulant (57.3%) and 415 were not (42.7%). The mean ages of patients discharged on anticoagulation and off anticoagulation were 75.6 years (+/-13.0 years) and 79.5 years (+/-10.8 years) respectively (p<.0001). Fifty-five patients experienced a major bleed within 1 year following hospital discharge (5.6%). Of these patients, 29 were not discharged on an anticoagulant, and 26 were discharged on an anticoagulant (p=0.12). The majority of the major bleeds were intracranial (n=33), and most of these occurred in patients discharged off anticoagulation (n=23) (p< 0.001). One-year post-discharge thrombotic complications included deep venous thrombus (DVT) (n= 13), pulmonary embolism (PE) (n=9), cerebrovascular accident or transient ischemic attack (CVA/TIA) (n=31), and acute coronary syndrome (ACS) (n=16). The majority of the thrombotic events occurred in patients who were discharged without an anticoagulant (n=45, 65.2%). Twenty-two patients (5.3%) who were discharged without an anticoagulant had CVA/TIA within 1 year following discharge compared to 9 patients discharged on an anticoagulant (1.6%) (p<.001). There were 405 patients (41.8%) readmitted to the hospital within 1 year following discharge from the index trauma hospitalization. Of these patients, 219 were discharged from the index trauma hospitalization on an anticoagulant (54.1%), and 186 were discharged without an anticoagulant (45.9%) (p=0.07). There were 147 readmission patients documented as having at least one hospital readmission related to trauma, and among those patients, 36 had multiple readmissions for trauma (8.9% of all readmitted patients).
Conclusions: After admission for trauma while on anticoagulation, patients discharged on anticoagulation had decreased risk of stroke, and they did not have increased risk of major bleeding events post-discharge compared to patients discharged off anticoagulation. There were similar readmission rates between the two groups, including readmissions for trauma. These outcomes, along with individual patient priorities, should be considered in anticoagulant decision-making when trauma occurs.