Background: Healthcare networks not only address medical needs but also connect patients with critical social support services. Socioeconomic factors significantly influence both healthcare utilization and outcomes, and screening for health-related social needs (HRSN) has improved outcomes, particularly among at-risk patients (Hood 2016; Gulati 2024). Despite these benefits, widespread implementation lagged until January 2024, when the Centers for Medicare and Medicaid Services (CMS) mandated universal HRSN screening for hospitalized patients (Schoenbaum 2023). CMS mandates screening in five domains: food insecurity, interpersonal safety, housing instability, transportation barriers, and utilities insecurity, but limited guidance on standardized methodologies has led to variability in implementation (Boch 2020). Additionally, there are no validated methods to assess screening quality (DeMarchis 2023). At our institution, all hospitalized patients are screened for HRSN on admission by nurses. Some of these patients may also be screened by Community Health Workers (CHWs) with or without medical students as part of a preclinical course which pre-dated the CMS mandate. This study evaluates the implementation of CMS-mandated HRSN screening at Jefferson Health, comparing screening outcomes between nurses and CHW/medical students for Hospital Medicine patients.
Methods: We conducted a retrospective study of HRSN screening results for 152 patients discharged from Thomas Jefferson University Hospital’s Division of Hospital Medicine between 1/1/2024 and 6/30/2024. Inclusion required completed HRSN screens by both a nurse and a CHW/medical student in Epic medical records. Screens overlapped in six domains: food, housing, utilities, healthcare, transportation, and financial burden of doctor’s visits. Statistical analyses assessed documentation rates and concordance between screeners.
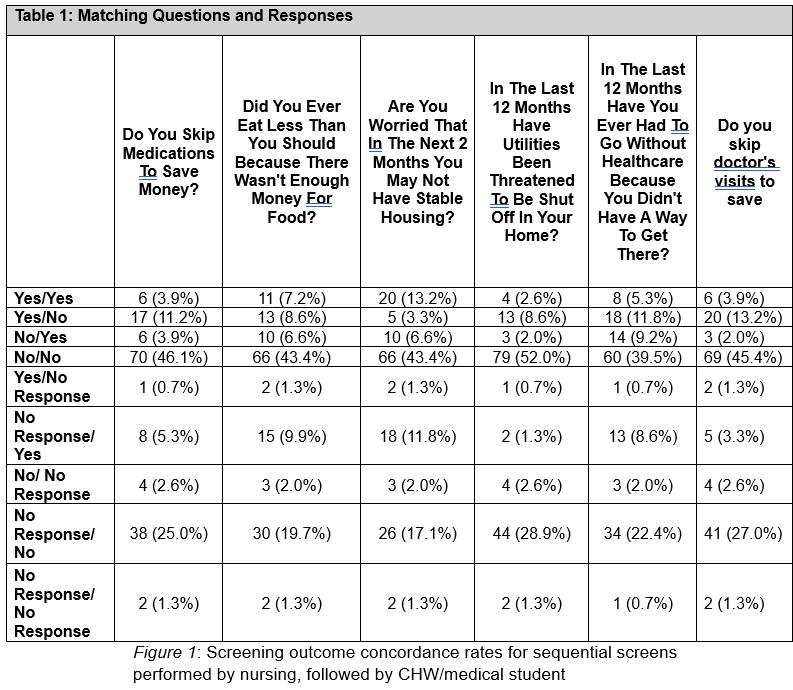
Results: Nurses completed HRSN screenings in 69% of cases, compared to 85% by CHW/medical students. When both assessed the same social domain, discordance occurred in 22% of cases – highest for transportation insecurity (32%) and lowest for housing instability (15%). Across all screens, 77% of patients reported at least one positive HRSN domain, with housing instability having the highest positivity rate (36.2%) and utilities the lowest (14.8%).
Conclusions: High discordance rates underscore the need for standardized HRSN screening practices and suggest there may be value to conducting multiple screens per patient. Reliance on electronic documentation limits this study, as it may not fully capture screening processes. Further research should focus on validating and standardizing HRSN screening to enhance consistency and equity in addressing patients’ social needs.