Background: Over 1 million patients are hospitalized in the United States yearly for pneumonia, of which 40% develop parapneumonic effusion. Left untreated, these effusions can progress to complex effusions requiring more invasive treatment, including tube thoracostomy and surgical decortication, increasing hospital length of stay and overall morbidity. In patients with complex parapneumonic effusion, intrapleural lytic enzyme therapy (IPET) including DNAse and TPA has been shown to reduce the need for surgery and overall length of stay. While early ultrasound (US) and thoracentesis can both treat and risk stratify effusions to identify patients who would benefit from IPET, the diagnosis and treatment of parapneumonic effusion often involves multiple services, which can lead to fragmentation and delays in care.
Purpose: We aimed to minimize delays in diagnosis and shorten length of stay for patients with parapneumonic effusion by creating a multidisciplinary Complex Effusion Management Team (CEMT), combining Hospital Medicine and Pulmonary expertise with standardized workflows for diagnosis and management.
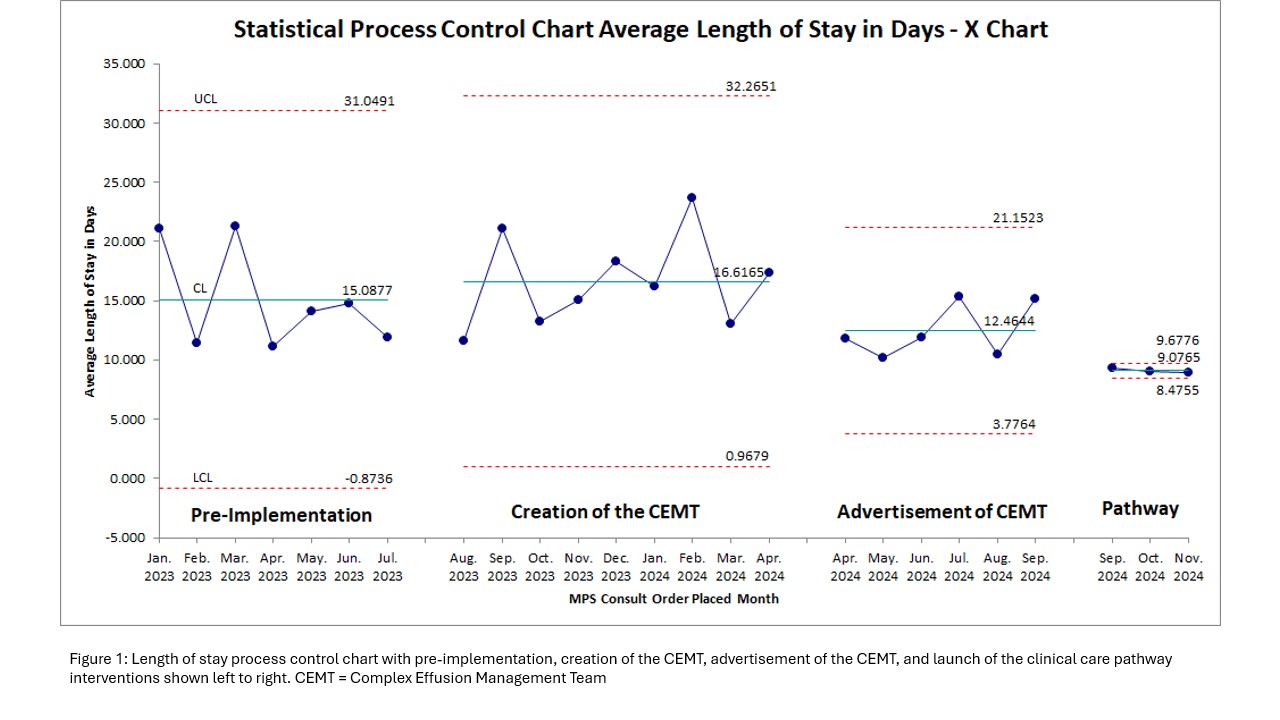
Description: The CEMT consists of our Medicine Procedure Service (MPS) and Pulmonary Consult Service (PCS). The MPS is staffed by Hospitalists with experience in US, thoracentesis, and IPET administration. The PCS is staffed by Pulmonary physicians with experience in pleural space management and tube thoracostomy. The CEMT launched on August 1, 2023 with MPS and PCS leadership creating a standardized workflow for patients with new effusion or lower lobe consolidation on chest radiograph. MPS is consulted first for lung ultrasound and possible thoracentesis. In effusions that appear complex on US or have exudative features, PCS is consulted for guidance on further management including tube thoracostomy placement if indicated. MPS then administers IPET and confers with PCS daily to optimize pleural space management. A campaign was launched in April 2024 to improve visibility of the CEMT including email advertisement and presentations at hospital medicine division meetings. In September 2024, we deployed a clinical pathway for new pleural effusions to direct teams to consult the CEMT. Following these interventions, the average length of stay for patients with parapneumonic effusion decreased from 15 days to 10 days with narrowing of both the upper and lower control limits, indicating a reduction in variability of the process (Figure 1).
Conclusions: Deployment of a CEMT, which centralized Hospital Medicine and Pulmonary experts allowing collaboration and co-development of clinical pathways to standardize care, was associated with both a significant reduction in length of stay and less variability in length of stay.