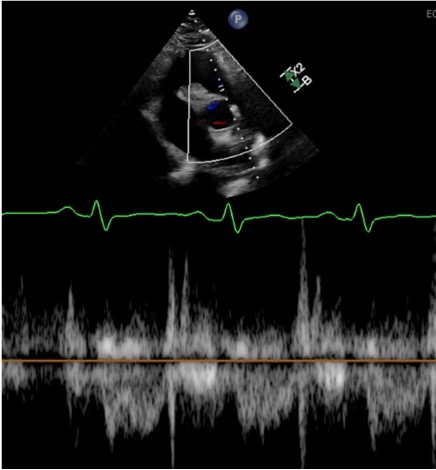
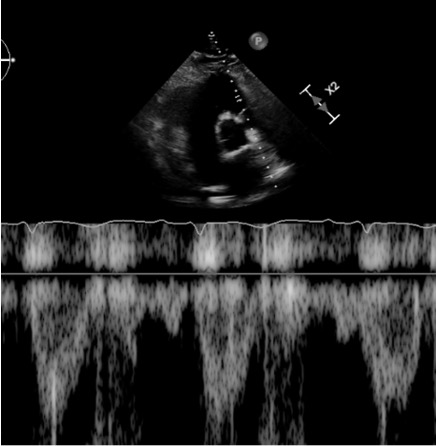
Case Presentation: A 62-year-old man presented to the emergency department with chest pain and dyspnea after recently driving from Michigan to Florida. In the ER, he was hypertensive and tachypneic with normal saturations. EKG showed sinus tachycardia with a classic S1Q3T3 pattern. Labs revealed an elevated D-dimer and troponin. CTA chest revealed a large saddle pulmonary embolism (PE) at the bifurcation of the pulmonary artery trunk into the right and left main pulmonary arteries, filling defects throughout both lungs and signs of right ventricular (RV) strain. Transthoracic echocardiogram (TTE) revealed early systolic notching of the right ventricular outflow tract (RVOT) envelope, dilated right atrium and ventricle, moderate to severely impaired RV function, and a right ventricular systolic pressure (RVSP) of 38 mm Hg (Figure 1). He emergently underwent bilateral suction thrombectomy with a moderate amount of thrombus extracted from the left and right pulmonary arteries. The end of the procedure was complicated by brief pulseless electrical activity requiring CPR with one round of chest compressions before ROSC. A stat TTE revealed a large, serpentine thrombus in transit between the right atrial and ventricle, for which tissue plasminogen activator (tPA) was given. Repeat CTA chest showed improvement in PE and the development of hemopericardium. TTE confirmed the effusion and tamponade physiology. The patient underwent pericardiocentesis for cardiac tamponade with eventual improvement in hypoxia and hemodynamics. Repeat TTE showed the resolution of early systolic notching of the RVOT waveform, mild to moderately impaired right ventricle systolic function, bi-atrial dilation, mild to moderate mitral regurgitation, moderate tricuspid regurgitation, mild pulmonic valve regurgitation, and an increase in RVSP to 42 mm Hg (Figure 2). Hypercoagulopathy workup found a heterozygous Factor V Leiden mutation, and long-term anticoagulation with apixaban was implemented.
Discussion: We present a case of high-risk submassive PE in which systolic notching of the right ventricular outflow tract resolved after thrombectomy and tPA. Echocardiographic findings correlating to RV function, such as RV dilation, right ventricular systolic pressure (RVSP), and tricuspid annular plane systolic excursion (TAPSE), lack specificity for elevated pulmonary vascular resistance (PVR). Notching of the pulse wave doppler envelope at the RVOT is a specific finding for elevated PVR in pulmonary arterial hypertension and is increasingly recognized as a tool in acute pulmonary embolism.1,2,3 Early systolic notching of the RVOT waveform may be more specific in acute PE than other more cited findings, such as the 60/60 sign.1 This finding may indicate that the resolution of RVOT notching is a useful tool for assessing response and risk after treatment of acute pulmonary embolism. There is a lack of literature describing the utility of monitoring the resolution of RVOT notching when assessing response to interventions in RV failure.
Conclusions: This case highlights the value of the shape of the RVOT envelope when diagnosing and assessing response to treatment in acute PE. Failure to resolve RVOT notching may prove to be an indication of inadequate response to treatment, and further studies are warranted. This case also highlights RVSP’s limitations and lack of specificity since the patient’s RVSP increased after hemodynamic improvement.