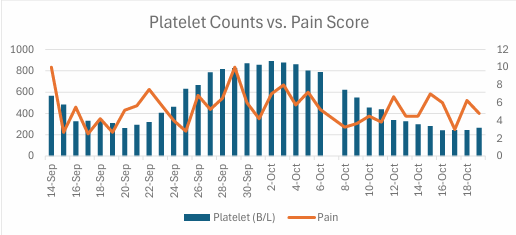
Case Presentation: 42-year-old female with past medical history of type 1 diabetes mellitus complicated by recurrent diabetic ketoacidosis (DKA), coronary artery disease (CAD), peripheral arterial disease (PAD), and blue toe syndrome (BTS) complicated by recent amputations of her right 1-2 toes, presented to an outside hospital (OSH) in DKA. She was also septic with methicillin-susceptible Staphylococcus aureus bacteremia. An echodensity was found on transesophageal echocardiogram (TEE), suspicious for vegetation. She had increasing pain in her right third toe with ischemic changes, including ulceration and discoloration, initially thought to be secondary to septic emboli. She was transferred to our hospital for further evaluation. A cardiac MRI did not visualize the TEE finding, ruling out septic emboli. Imaging and ultrasound studies were consistent with BTS. Prior hypercoagulable workup was negative. The team noted her increasing platelet count correlated with worsening toe pain. Thrombocytosis in a patient with underlying PAD and tobacco use was considered as a cause of microvascular thrombosis. Cephalosporin-induced thrombocytosis was considered but ruled out as she had prior episodes without cephalosporin exposure. Essential thrombocytosis was ruled out with genetic testing. Further, detailed history revealed her hospitalizations often correlated with menstrual periods accompanied by worsening menorrhagia in the preceding decade. This information was correlated with severe microcytic anemia and severely depressed ferritin consistent with iron deficiency with reactive thrombocytosis. On further review, she had had a similar degree of iron-deficient anemia and thrombocytosis during a prior hospitalization that concluded with her amputations. Though clinicians at that time had attributed her BTS to atherosclerotic emboli, our team wondered if thrombocytosis was the cause. A literature review found a single international case report of a similar scenario in which a patient responded to intravenous iron repletion. We trialed the same course, with improvement in her platelets and pain, suggesting confirmation of our pathophysiologic hypothesis.
Discussion: BTS is usually an end-arterial embolic phenomenon. It is acutely painful and often presents with discolored toes. Outcomes vary: some resolve completely, others develop chronic pain or progress to gangrene and require amputation. Thrombocytosis is a rare cause of BTS. As BTS is a secondary phenomenon, targeting the underlying cause is critical to prevent its worst outcomes. In our case, identifying severe iron-deficient anemia secondary to progressive menorrhagia leading to reactive thrombocytosis provided a therapeutic target. While there was not perfect correlation between pain scores and opiate needs (MME) with platelet trends, discontinuation of acetaminophen and pregabalin when the patient returned to the OSH (10/5) and tissue manipulation there likely explains the blunting of pain improvement.
Conclusions: This case highlights the importance of hospitalists taking detailed histories, methodically reviewing chart data, and applying literature at the bedside to broaden differentials, prevent diagnostic anchoring, explain otherwise unexplained laboratory abnormalities, and improve targeted therapies. We are cautiously optimistic that this approach averted the amputation of a third toe for this patient and offers a template to help future patients not responding to treatment.