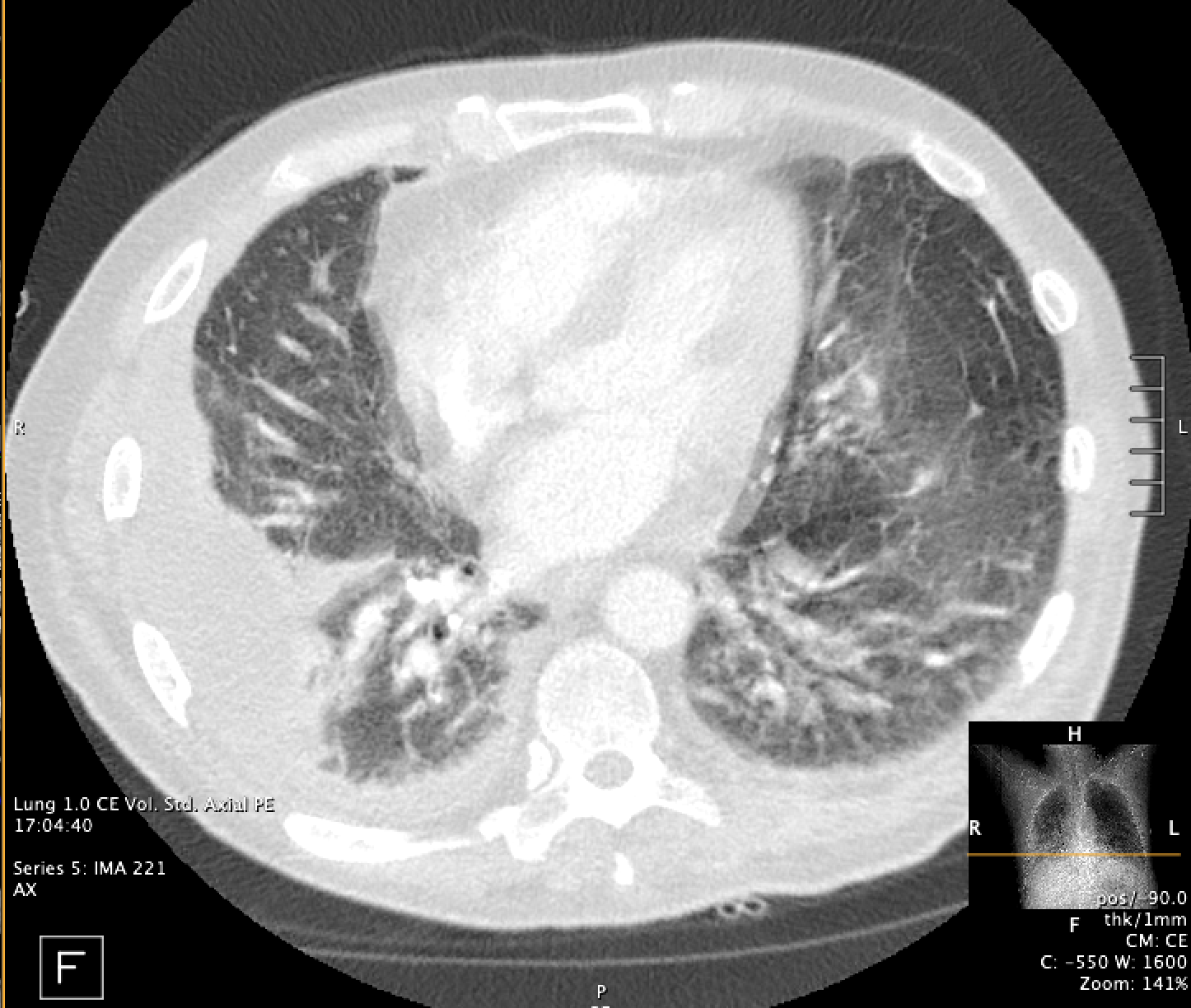
Case Presentation: 50 year old male with PMH significant for seizure disorder (on Keppra) and COPD (not on home oxygen) presenting with weakness, fatigue, dyspnea on exertion, and 50-pound weight loss over four months. During this admission, he was found to have acute hypoxic respiratory failure secondary to right basilar pneumonia with small right pleural effusion. He was treated with IV cefepime and subsequently discharged on 4 liters of oxygen and Levaquin to complete a seven-day course. However, his symptoms persisted over the next five weeks, resulting in re-admission. He was now found to have sepsis and acute on chronic hypoxic respiratory failure requiring escalation to high flow nasal canula secondary to loculated moderate right pleural effusion. He was restarted on broad spectrum antibiotics and underwent chest tube placement which was subsequently removed after 3 days due to tapering output. Thora fluid confirmed parapneumonic effusion and gram stain/ culture was negative. After chest tube removal, he started fevering daily as high as 102.7 F despite being on broad spectrum antibiotics. Imaging revealed improved persistent right loculated pleural effusion and non-specific abdominal lymphadenopathy. He subsequently became pancytopenic, including leukopenia and neutropenia. Extensive workup ultimately revealed ANA 1:1280, hematophagocytes in the pleural fluid, markedly elevated ferritin at 32,000, CD25 elevation, and decreased NK cell count (activity could not be performed). Repeat thora showed empyema. Karius was positive for PJP. He was started on Bactrim and dexamethasone with resolution of his symptoms.
Discussion: While his ANA is concerning for an underlying autoimmune condition, it is thought that infection ultimately triggered his HLH as his symptoms improved with antibiotics and steroids rather than anakinra which is the treatment of autoimmune related HLH, also called macrophage activation syndrome (in addition to steroids).
Conclusions: HLH is an exceedingly rare cause of fever in adults. PJP in a relatively healthy individual is unheard of. This case highlights the importance of HLH as a cause of persistent fevers (especially given its high mortality rate), and how karius can be helpful in diagnosis when all other diagnostics (lab, sputum, imaging, fluid studies) were negative in illuminating the trigger for this patient’s HLH.
.png)