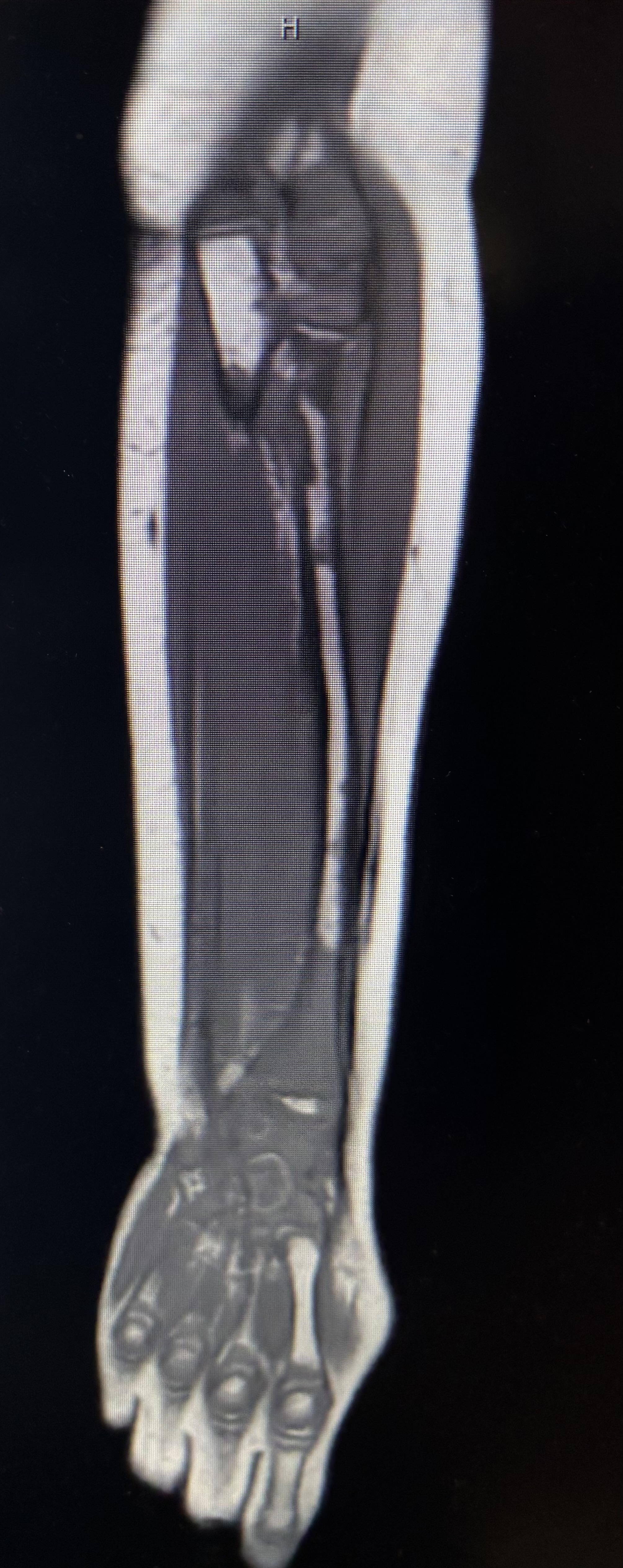
Case Presentation: A 7-year-old female presented with 3 days of bilateral knee pain and 1 day of left wrist pain and swelling. Knee pain resolved 1 day prior to presentation at which point left wrist symptoms started. No fevers, recent illnesses, or history of trauma. History notable for Acute Myeloid Leukemia (AML) diagnosed at 4 years of age now in remission after bone marrow transplant 3 years prior. Vital signs were normal, and she was overall well appearing in no acute distress. Left wrist was mildly swollen with pain on both palpation and flexion with overall decreased range of motion. Other joints were without swelling, erythema, effusion, tenderness and had full range of motion. Initial labs showed unremarkable CBC, CMP, procalcitonin, CRP, and uric acid. ESR mildly elevated at 20 mm/hr. LDH elevated at 464 U/L. Left wrist Xray showed abnormal demineralization of the distal ulnar metaphyseal cortex. Orthopedic surgery recommended MRI to evaluate for osteomyelitis versus septic arthritis. MRI left wrist showed multifocal osseous areas of T1 hypo-intensity with corresponding T2 hyperintensity within the visualized bones of the left upper extremity as well as partially included pelvis and left lower extremity. There was a small radiocarpal and intercarpal joint effusion with superficial and deep soft tissue swelling at the level of the wrist and proximal hand without drainable collection or abscess. Oncology was consulted due to the concerning nature of MRI for malignancy, prompting bone marrow biopsy. This revealed 42.5% blasts on aspirate smear and normocellular marrow with limited areas of regenerating trilineage hematopoiesis. Peripheral blood morphology from initial CBC showed very rare circulating blasts with similar morphology to marrow aspirate; red cells and platelets showed no significant morphologic abnormalities. The patient was diagnosed with relapsed AML and swiftly started chemotherapy.
Discussion: Late relapse of AML after allogeneic stem cell transplant is uncommon, occurring in approximately 7% of patients (1). Additionally, a younger age at time of diagnosis and transplant is associated with a lower risk of relapse (2). Therefore, differential diagnosis was broad including reactive arthritis, septic arthritis, osteomyelitis, and relapsed AML with leading diagnoses being more infectious in nature rather than oncologic. However, a recent study showed that AML can present as musculoskeletal pain in approximately 29% of patients under the age of 15, purposing that more consideration should be given to oncologic etiology in patients with joint pain, particularly if the patient also has elevated LDH (3).
Conclusions: Despite the decreased risk of relapse in our patient given her age and being several years out from bone marrow transplant, this case highlights the importance of a broad differential and use of MR imaging to evaluate infection vs. oncologic processes in patients with a history of AML presenting with musculoskeletal symptoms.