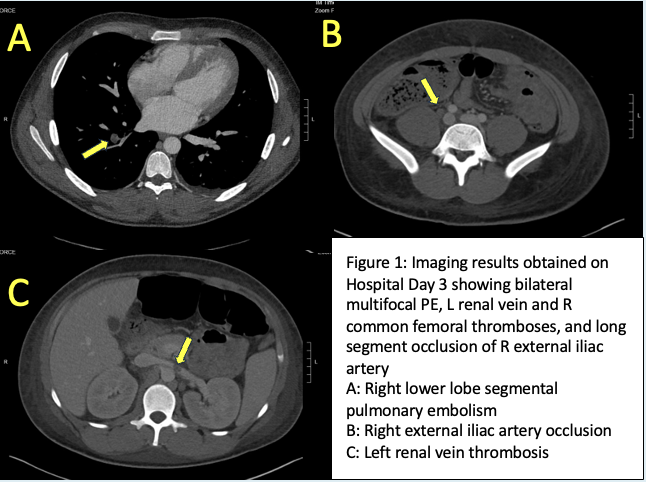
Case Presentation: A healthy 15-year-old male developed cough, nasal congestion, and abdominal pain. After several days, he presented to the hospital with worsening pain and emesis. He was febrile to 100.4 degrees Fahrenheit, with a heart rate of 121 beats per minute and a respiratory rate of 27 breaths per minute. He appeared pale and in mild discomfort. His abdomen was distended and diffusely tender without peritoneal signs. Laboratory data showed a hemoglobin of 6.6 g/dL, normal white-blood-cell and platelet counts, creatinine 1.1 mg/dL, and albumin 1.7 g/dL. Spot urine protein-to-creatinine ratio was markedly elevated at 10.4. Lactate dehydrogenase was elevated at 349 U/L, haptoglobin was low at 11 mg/dL, and the direct antiglobulin test was strongly positive with pan-agglutinins. A throat swab was positive for group A beta-hemolytic streptococcus. Further workup revealed positive lupus anticoagulant, anti-beta2-glycoprotein 1 antibodies, and anti-cardiolipin antibodies. Contrast-enhanced computed tomography of the chest, abdomen, and pelvis revealed acute bilateral pulmonary emboli and multifocal thrombi of the left renal vein, right common femoral vein, and right external iliac artery. The patient received 1 unit of packed red blood cells and five days of methylprednisolone and intravenous immunoglobulin for autoimmune hemolytic anemia. He was treated for probable catastrophic antiphospholipid syndrome (CAPS) with intravenous heparin and bridged to warfarin. He was initiated on rituximab and hydroxychloroquine, and transitioned to an oral prednisone taper. He received a course of ceftriaxone for possible streptococcal pharyngitis and azithromycin for cold agglutinin disease. His hemoglobin stabilized and renal function normalized by discharge on hospital day 20.
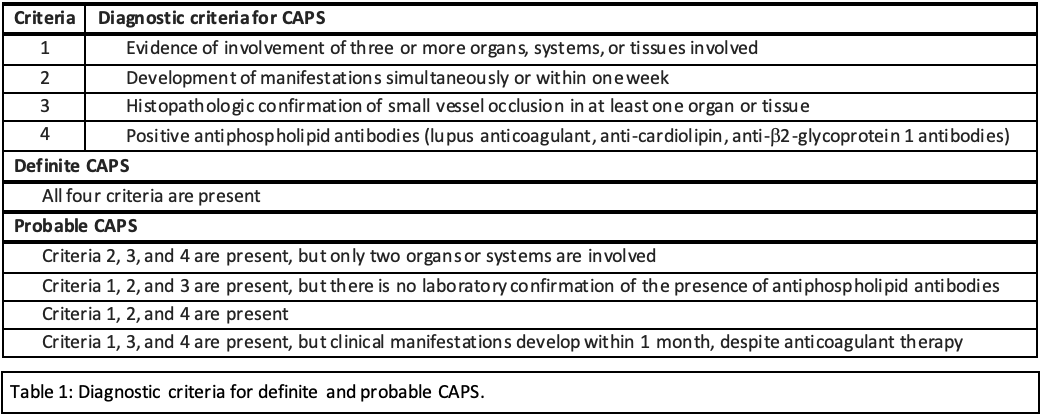
Discussion: CAPS is a rare complication of antiphospholipid syndrome (APS) characterized by rapid, widespread microvascular thromboses which may lead to multiorgan failure and death. Since infection is the most common trigger, symptoms may be attributed to self-limited illness and diagnosis can be delayed. Ultimately, our patient’s unexplained anemia, hypoalbuminemia, and proteinuria prompted the necessary diagnostic tests and specialty consultations. CAPS is classified as definite or probable (Table 1). Our patient met criteria for probable CAPS based on rapid development of thromboses, involvement of the renal, pulmonary, and hematologic systems, and the presence of antiphospholipid antibodies. He did not fulfill the fourth criterion of histopathological confirmation since renal biopsy was deferred due to anasarca and bleeding risk.
Conclusions: The evaluation of a child with CAPS can be challenging, with potentially devastating consequences from delayed or missed diagnosis. The pediatric hospitalist must maintain a high index of suspicion for rare conditions when no clear unifying diagnosis exists. In particular, autoimmune or rheumatologic disease should be considered strongly in cases of multiorgan involvement and hematologic abnormalities.